Thillagavathie Pillay, Sarah E Seaton, Miaoqing Yang, Vasiliki Bountziouka, Victor Banda, Helen Campbell, Kelvin Dawson, Bradley N Manktelow, Elizabeth S Draper, Neena Modi, Elaine M Boyle, Oliver Rivero-Arias
{"title":"改善英国早产儿的预后:出生地重要吗?OPTI-PREM是一项全国性队列研究。","authors":"Thillagavathie Pillay, Sarah E Seaton, Miaoqing Yang, Vasiliki Bountziouka, Victor Banda, Helen Campbell, Kelvin Dawson, Bradley N Manktelow, Elizabeth S Draper, Neena Modi, Elaine M Boyle, Oliver Rivero-Arias","doi":"10.1136/archdischild-2024-327474","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Babies born between 27<sup>+0</sup> and 31<sup>+6</sup> weeks of gestation contribute substantially towards infant mortality and morbidity. In England, their care is delivered in maternity services colocated with highly specialised neonatal intensive care units (NICU) or less specialised local neonatal units (LNU). We investigated whether birth setting offered survival and/or morbidity advantages to inform National Health Service delivery.</p><p><strong>Design: </strong>Retrospective national cohort study.</p><p><strong>Setting: </strong>LNU, NICU, England.</p><p><strong>Patients: </strong>UK National Neonatal Research Database whole population data for births between 27<sup>+0</sup> and 31<sup>+6</sup> weeks of gestation, discharged from/died within neonatal units between 1 January 2014 and 31 December 2018. We linked baby-level data to mortality information from the Office for National Statistics.</p><p><strong>Outcome measures: </strong>Death during neonatal care, up to 1 year (infant mortality), surgically treated necrotising enterocolitis, retinopathy of prematurity, severe brain injury (SBI), bronchopulmonary dysplasia.</p><p><strong>Intervention: </strong>Birth in NICU versus LNU setting. We used an instrumental variable (maternal excess travel time between the nearest NICU and LNU) estimation approach to determine treatment effect.</p><p><strong>Results: </strong>Of 18 847 babies (NICU: 10 379; LNU: 8468), 574 died in NICU/LNU care, and 121 postdischarge (infant mortality 3.7%). We found no effect of birth setting on neonatal or infant mortality. Significantly more babies born into LNU settings experienced SBI (mean difference -1.1% (99% CI -2.2% to -0.1%)). This was attenuated after excluding births at 27 weeks, and early postnatal transfers.</p><p><strong>Conclusions: </strong>In England, LNU teams should use clinical judgement, risk assessing benefits of transfer versus risk of SBI for preterm births at 27 weeks of gestation. 28 weeks of gestation is a safe threshold for preterm birth in either NICU/LNU settings.</p><p><strong>Trial registration number: </strong>NCT02994849/ISRCTN74230187.</p>","PeriodicalId":8177,"journal":{"name":"Archives of Disease in Childhood - Fetal and Neonatal Edition","volume":" ","pages":"444-451"},"PeriodicalIF":3.6000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12418565/pdf/","citationCount":"0","resultStr":"{\"title\":\"Improving outcomes for very preterm babies in England: does place of birth matter? Findings from OPTI-PREM, a national cohort study.\",\"authors\":\"Thillagavathie Pillay, Sarah E Seaton, Miaoqing Yang, Vasiliki Bountziouka, Victor Banda, Helen Campbell, Kelvin Dawson, Bradley N Manktelow, Elizabeth S Draper, Neena Modi, Elaine M Boyle, Oliver Rivero-Arias\",\"doi\":\"10.1136/archdischild-2024-327474\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Babies born between 27<sup>+0</sup> and 31<sup>+6</sup> weeks of gestation contribute substantially towards infant mortality and morbidity. In England, their care is delivered in maternity services colocated with highly specialised neonatal intensive care units (NICU) or less specialised local neonatal units (LNU). We investigated whether birth setting offered survival and/or morbidity advantages to inform National Health Service delivery.</p><p><strong>Design: </strong>Retrospective national cohort study.</p><p><strong>Setting: </strong>LNU, NICU, England.</p><p><strong>Patients: </strong>UK National Neonatal Research Database whole population data for births between 27<sup>+0</sup> and 31<sup>+6</sup> weeks of gestation, discharged from/died within neonatal units between 1 January 2014 and 31 December 2018. We linked baby-level data to mortality information from the Office for National Statistics.</p><p><strong>Outcome measures: </strong>Death during neonatal care, up to 1 year (infant mortality), surgically treated necrotising enterocolitis, retinopathy of prematurity, severe brain injury (SBI), bronchopulmonary dysplasia.</p><p><strong>Intervention: </strong>Birth in NICU versus LNU setting. We used an instrumental variable (maternal excess travel time between the nearest NICU and LNU) estimation approach to determine treatment effect.</p><p><strong>Results: </strong>Of 18 847 babies (NICU: 10 379; LNU: 8468), 574 died in NICU/LNU care, and 121 postdischarge (infant mortality 3.7%). We found no effect of birth setting on neonatal or infant mortality. Significantly more babies born into LNU settings experienced SBI (mean difference -1.1% (99% CI -2.2% to -0.1%)). This was attenuated after excluding births at 27 weeks, and early postnatal transfers.</p><p><strong>Conclusions: </strong>In England, LNU teams should use clinical judgement, risk assessing benefits of transfer versus risk of SBI for preterm births at 27 weeks of gestation. 28 weeks of gestation is a safe threshold for preterm birth in either NICU/LNU settings.</p><p><strong>Trial registration number: </strong>NCT02994849/ISRCTN74230187.</p>\",\"PeriodicalId\":8177,\"journal\":{\"name\":\"Archives of Disease in Childhood - Fetal and Neonatal Edition\",\"volume\":\" \",\"pages\":\"444-451\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2025-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12418565/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archives of Disease in Childhood - Fetal and Neonatal Edition\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/archdischild-2024-327474\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Disease in Childhood - Fetal and Neonatal Edition","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/archdischild-2024-327474","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
摘要
目的:妊娠27+0至31+6周出生的婴儿对婴儿死亡率和发病率有重要影响。在英格兰,他们的护理是在产科服务中提供的,与高度专业化的新生儿重症监护病房(NICU)或不太专业的地方新生儿病房(lu)配合使用。我们调查了是否出生环境提供生存和/或发病率优势,以告知国家卫生服务提供。设计:回顾性国家队列研究。单位:英国LNU, NICU。患者:英国国家新生儿研究数据库2014年1月1日至2018年12月31日期间出生在妊娠27+0至31+6周之间、从新生儿病房出院/死亡的全人群数据。我们将婴儿水平的数据与国家统计局的死亡率信息联系起来。结局指标:新生儿护理期间死亡,最多1年(婴儿死亡率),手术治疗的坏死性小肠结肠炎,早产儿视网膜病变,严重脑损伤(SBI),支气管肺发育不良。干预:新生儿重症监护病房与新生儿重症监护病房的对比。我们使用工具变量(产妇在最近的NICU和LNU之间的额外旅行时间)估计方法来确定治疗效果。结果:18847例新生儿(NICU: 10379例;新生儿重症监护病房:8468人),574人在新生儿重症监护病房/新生儿重症监护病房死亡,121人在出院后死亡(婴儿死亡率3.7%)。我们没有发现出生环境对新生儿或婴儿死亡率的影响。在lu环境中出生的婴儿明显更多地经历了SBI(平均差异-1.1% (99% CI -2.2%至-0.1%))。在排除27周分娩和早期产后转移后,这种情况有所减弱。结论:在英国,LNU团队应该使用临床判断,风险评估转移的益处与27周妊娠早产儿SBI的风险。无论是NICU还是lu,妊娠28周都是早产的安全阈值。试验注册号:NCT02994849/ISRCTN74230187。
Improving outcomes for very preterm babies in England: does place of birth matter? Findings from OPTI-PREM, a national cohort study.
Objective: Babies born between 27+0 and 31+6 weeks of gestation contribute substantially towards infant mortality and morbidity. In England, their care is delivered in maternity services colocated with highly specialised neonatal intensive care units (NICU) or less specialised local neonatal units (LNU). We investigated whether birth setting offered survival and/or morbidity advantages to inform National Health Service delivery.
Design: Retrospective national cohort study.
Setting: LNU, NICU, England.
Patients: UK National Neonatal Research Database whole population data for births between 27+0 and 31+6 weeks of gestation, discharged from/died within neonatal units between 1 January 2014 and 31 December 2018. We linked baby-level data to mortality information from the Office for National Statistics.
Outcome measures: Death during neonatal care, up to 1 year (infant mortality), surgically treated necrotising enterocolitis, retinopathy of prematurity, severe brain injury (SBI), bronchopulmonary dysplasia.
Intervention: Birth in NICU versus LNU setting. We used an instrumental variable (maternal excess travel time between the nearest NICU and LNU) estimation approach to determine treatment effect.
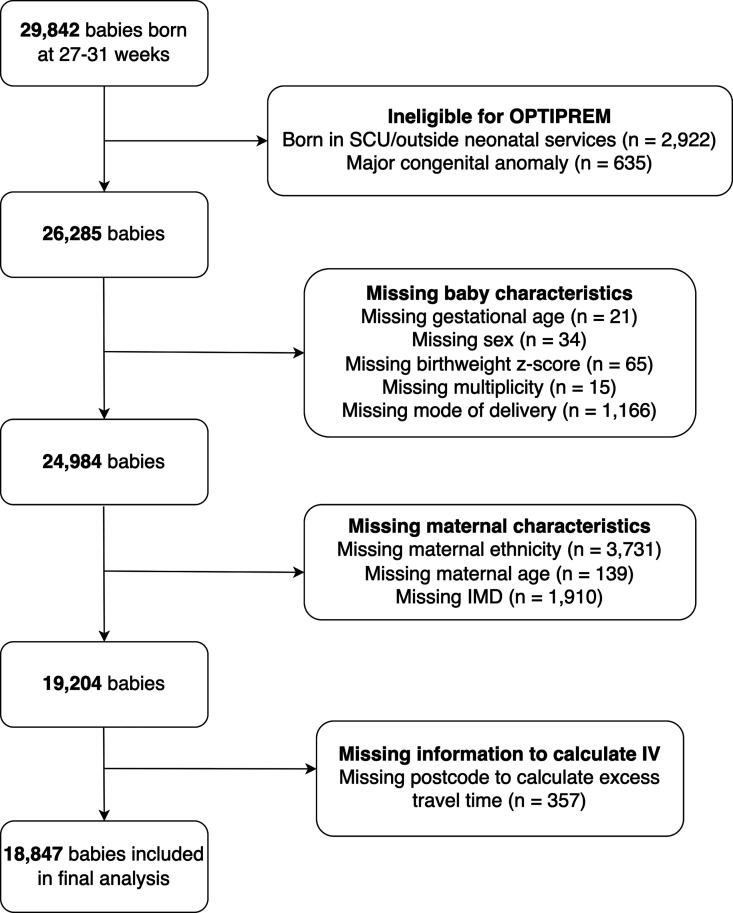
Results: Of 18 847 babies (NICU: 10 379; LNU: 8468), 574 died in NICU/LNU care, and 121 postdischarge (infant mortality 3.7%). We found no effect of birth setting on neonatal or infant mortality. Significantly more babies born into LNU settings experienced SBI (mean difference -1.1% (99% CI -2.2% to -0.1%)). This was attenuated after excluding births at 27 weeks, and early postnatal transfers.
Conclusions: In England, LNU teams should use clinical judgement, risk assessing benefits of transfer versus risk of SBI for preterm births at 27 weeks of gestation. 28 weeks of gestation is a safe threshold for preterm birth in either NICU/LNU settings.
期刊介绍:
Archives of Disease in Childhood is an international peer review journal that aims to keep paediatricians and others up to date with advances in the diagnosis and treatment of childhood diseases as well as advocacy issues such as child protection. It focuses on all aspects of child health and disease from the perinatal period (in the Fetal and Neonatal edition) through to adolescence. ADC includes original research reports, commentaries, reviews of clinical and policy issues, and evidence reports. Areas covered include: community child health, public health, epidemiology, acute paediatrics, advocacy, and ethics.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
