Andrew A Lawson, Kae Watanabe, Lindsay Griffin, Christina Laternser, Michael Markl, Cynthia K Rigsby, Joshua D Robinson, Nazia Husain
{"title":"多参数心血管磁共振与儿童心脏移植受者的预后相关。","authors":"Andrew A Lawson, Kae Watanabe, Lindsay Griffin, Christina Laternser, Michael Markl, Cynthia K Rigsby, Joshua D Robinson, Nazia Husain","doi":"10.1016/j.jocmr.2024.101138","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Multiparametric cardiovascular magnetic resonance (CMR) has an emerging role in non-invasive surveillance of pediatric heart transplant recipients (PHTR). Higher myocardial T2, higher extracellular volume fraction (ECV), and late gadolinium enhancement (LGE) have been associated with adverse clinical outcomes in adult heart transplant recipients. The purpose of this study was to investigate the prognostic value of CMR-derived T1 and T2 mapping, ECV, and LGE for clinical outcomes in PHTR.</p><p><strong>Methods: </strong>We performed a single-center, retrospective chart review of consecutive, gadolinium-enhanced CMR studies in PHTR over a 7.5-year period, excluding follow-up studies. Standard CMR ventricular volume and function analysis, T1 mapping with ECV, T2 mapping, and LGE assessment were performed. The composite outcome included cardiac death, non-cardiac death, re-transplantation, and cardiac hospitalization.</p><p><strong>Results: </strong>Among 113 PHTR, mean age was 13.0 ± 5.1 years, with 6.0 ± 4.0 years since transplant. The indication for CMR was surveillance in 79%. Mean native T1 was 1050 ± 48 ms, T2 49.2 ± 3.9 ms, and ECV 29.7 ± 4.5%. Left ventricular LGE was present in 37% (42/113) and right ventricular LGE in 3.5% (4/113). The mean follow-up time was 2.3 years and median was 1.4 years. Cardiac death occurred in 2% (2/113), re-transplantation in 4% (4/113), and cardiac hospitalization in 22% (25/113). Non-cardiac death did not occur. Using Kaplan-Meier analysis, high T1 (≥1061 ms), T2 (≥50.0 ms), and ECV (≥31.4%) were each associated with decreased freedom from the composite outcome in follow-up. In univariable Cox regression analyses, high T1 was associated with increased risk of the composite outcome (hazard ratios [HR] 4.0, 95% confidence interval [CI] 1.7-9.2, p = 0.001), as were high T2 (HR 2.8, 95% CI 1.1-7.1, p = 0.026), and high ECV (HR 3.5, 95% CI 1.5-8.1, p = 0.004).</p><p><strong>Conclusion: </strong>T1 and T2 mapping are associated with early differences in adverse cardiac events in PHTR. These data suggest a role for a multicenter study with a longer follow-up duration.</p>","PeriodicalId":15221,"journal":{"name":"Journal of Cardiovascular Magnetic Resonance","volume":" ","pages":"101138"},"PeriodicalIF":6.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11783449/pdf/","citationCount":"0","resultStr":"{\"title\":\"Multiparametric cardiovascular magnetic resonance is associated with outcomes in pediatric heart transplant recipients.\",\"authors\":\"Andrew A Lawson, Kae Watanabe, Lindsay Griffin, Christina Laternser, Michael Markl, Cynthia K Rigsby, Joshua D Robinson, Nazia Husain\",\"doi\":\"10.1016/j.jocmr.2024.101138\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Multiparametric cardiovascular magnetic resonance (CMR) has an emerging role in non-invasive surveillance of pediatric heart transplant recipients (PHTR). Higher myocardial T2, higher extracellular volume fraction (ECV), and late gadolinium enhancement (LGE) have been associated with adverse clinical outcomes in adult heart transplant recipients. The purpose of this study was to investigate the prognostic value of CMR-derived T1 and T2 mapping, ECV, and LGE for clinical outcomes in PHTR.</p><p><strong>Methods: </strong>We performed a single-center, retrospective chart review of consecutive, gadolinium-enhanced CMR studies in PHTR over a 7.5-year period, excluding follow-up studies. Standard CMR ventricular volume and function analysis, T1 mapping with ECV, T2 mapping, and LGE assessment were performed. The composite outcome included cardiac death, non-cardiac death, re-transplantation, and cardiac hospitalization.</p><p><strong>Results: </strong>Among 113 PHTR, mean age was 13.0 ± 5.1 years, with 6.0 ± 4.0 years since transplant. The indication for CMR was surveillance in 79%. Mean native T1 was 1050 ± 48 ms, T2 49.2 ± 3.9 ms, and ECV 29.7 ± 4.5%. Left ventricular LGE was present in 37% (42/113) and right ventricular LGE in 3.5% (4/113). The mean follow-up time was 2.3 years and median was 1.4 years. Cardiac death occurred in 2% (2/113), re-transplantation in 4% (4/113), and cardiac hospitalization in 22% (25/113). Non-cardiac death did not occur. Using Kaplan-Meier analysis, high T1 (≥1061 ms), T2 (≥50.0 ms), and ECV (≥31.4%) were each associated with decreased freedom from the composite outcome in follow-up. In univariable Cox regression analyses, high T1 was associated with increased risk of the composite outcome (hazard ratios [HR] 4.0, 95% confidence interval [CI] 1.7-9.2, p = 0.001), as were high T2 (HR 2.8, 95% CI 1.1-7.1, p = 0.026), and high ECV (HR 3.5, 95% CI 1.5-8.1, p = 0.004).</p><p><strong>Conclusion: </strong>T1 and T2 mapping are associated with early differences in adverse cardiac events in PHTR. These data suggest a role for a multicenter study with a longer follow-up duration.</p>\",\"PeriodicalId\":15221,\"journal\":{\"name\":\"Journal of Cardiovascular Magnetic Resonance\",\"volume\":\" \",\"pages\":\"101138\"},\"PeriodicalIF\":6.1000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11783449/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular Magnetic Resonance\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1016/j.jocmr.2024.101138\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Magnetic Resonance","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.jocmr.2024.101138","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/25 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:多参数心血管磁共振(CMR)在儿童心脏移植受者(PHTR)的无创监测中发挥着新的作用。在成人心脏移植受者中,较高的心肌T2、较高的细胞外体积分数(ECV)和晚期钆增强(LGE)与不良临床结果相关。本研究的目的是探讨cmr衍生的T1和t2定位、ECV和LGE对PHTR临床结果的预后价值。方法:我们进行了一项单中心、回顾性的图表回顾,包括7.5年期间连续的、钆增强的PHTR CMR研究,不包括随访研究。进行标准CMR心室容积和功能分析、T1与ECV作图、T2作图和LGE评估。复合结局包括心源性死亡、非心源性死亡、再移植和心脏住院。结果:113例PHTR患者平均年龄为13.0±5.1岁,移植后平均年龄为6.0±4.0岁。79%的CMR适应症为监测。平均原生T1为1050±48ms;T2 49.2±3.9ms, ECV 29.7±4.5%。LV LGE占37% (42/113),RV LGE占3.5%(4/113)。平均随访时间2.3年,中位1.4年。心源性死亡占2%(2/113),再移植占4%(4/113),心脏住院占22%(25/113)。未发生非心源性死亡。Kaplan-Meier分析显示,高T1(≥1061ms)、高T2(≥50.0ms)和高ECV(≥31.4%)均与随访中复合结局的自由度降低相关。在单变量Cox回归分析中,高T1与复合结局的风险增加相关(HR 4.0, 95% CI 1.7-9.2, p=0.001),高T2 (HR 2.8, 95% CI 1.1-7.1, p=0.026)和高ECV (HR 3.5, 95% CI 1.5-8.1, p=0.004)。结论:T1和T2定位与PHTR患者不良心脏事件的早期差异有关。这些数据提示多中心研究和较长的随访时间的作用。
Multiparametric cardiovascular magnetic resonance is associated with outcomes in pediatric heart transplant recipients.
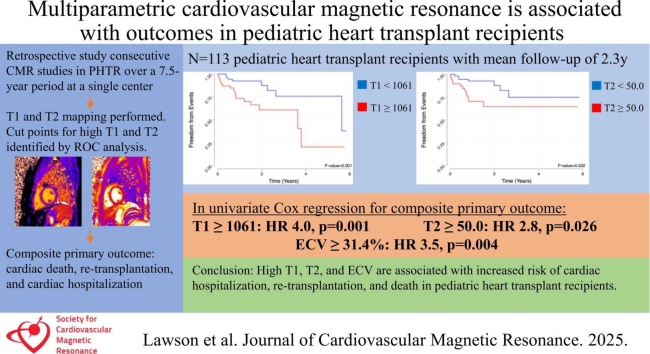
Background: Multiparametric cardiovascular magnetic resonance (CMR) has an emerging role in non-invasive surveillance of pediatric heart transplant recipients (PHTR). Higher myocardial T2, higher extracellular volume fraction (ECV), and late gadolinium enhancement (LGE) have been associated with adverse clinical outcomes in adult heart transplant recipients. The purpose of this study was to investigate the prognostic value of CMR-derived T1 and T2 mapping, ECV, and LGE for clinical outcomes in PHTR.
Methods: We performed a single-center, retrospective chart review of consecutive, gadolinium-enhanced CMR studies in PHTR over a 7.5-year period, excluding follow-up studies. Standard CMR ventricular volume and function analysis, T1 mapping with ECV, T2 mapping, and LGE assessment were performed. The composite outcome included cardiac death, non-cardiac death, re-transplantation, and cardiac hospitalization.
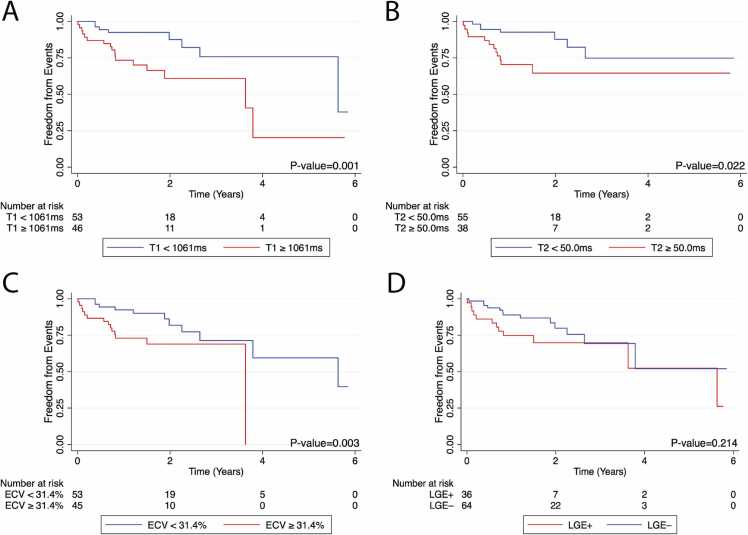
Results: Among 113 PHTR, mean age was 13.0 ± 5.1 years, with 6.0 ± 4.0 years since transplant. The indication for CMR was surveillance in 79%. Mean native T1 was 1050 ± 48 ms, T2 49.2 ± 3.9 ms, and ECV 29.7 ± 4.5%. Left ventricular LGE was present in 37% (42/113) and right ventricular LGE in 3.5% (4/113). The mean follow-up time was 2.3 years and median was 1.4 years. Cardiac death occurred in 2% (2/113), re-transplantation in 4% (4/113), and cardiac hospitalization in 22% (25/113). Non-cardiac death did not occur. Using Kaplan-Meier analysis, high T1 (≥1061 ms), T2 (≥50.0 ms), and ECV (≥31.4%) were each associated with decreased freedom from the composite outcome in follow-up. In univariable Cox regression analyses, high T1 was associated with increased risk of the composite outcome (hazard ratios [HR] 4.0, 95% confidence interval [CI] 1.7-9.2, p = 0.001), as were high T2 (HR 2.8, 95% CI 1.1-7.1, p = 0.026), and high ECV (HR 3.5, 95% CI 1.5-8.1, p = 0.004).
Conclusion: T1 and T2 mapping are associated with early differences in adverse cardiac events in PHTR. These data suggest a role for a multicenter study with a longer follow-up duration.
期刊介绍:
Journal of Cardiovascular Magnetic Resonance (JCMR) publishes high-quality articles on all aspects of basic, translational and clinical research on the design, development, manufacture, and evaluation of cardiovascular magnetic resonance (CMR) methods applied to the cardiovascular system. Topical areas include, but are not limited to:
New applications of magnetic resonance to improve the diagnostic strategies, risk stratification, characterization and management of diseases affecting the cardiovascular system.
New methods to enhance or accelerate image acquisition and data analysis.
Results of multicenter, or larger single-center studies that provide insight into the utility of CMR.
Basic biological perceptions derived by CMR methods.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
