Aya Fadel, Hussain Hussain, Robert J Hernandez, Amanda Marie Clichy Silva, Amir Agustin Estil-Las, Mohammad Hamad, Zahraa F Saadoon, Lamia Naseer, William C Sultan, Carla Sultan, Taylor Schnepp, Arumugam R Jayakumar
{"title":"神经梅毒诱发痴呆的机制:病理生理学的见解。","authors":"Aya Fadel, Hussain Hussain, Robert J Hernandez, Amanda Marie Clichy Silva, Amir Agustin Estil-Las, Mohammad Hamad, Zahraa F Saadoon, Lamia Naseer, William C Sultan, Carla Sultan, Taylor Schnepp, Arumugam R Jayakumar","doi":"10.3390/neurolint16060120","DOIUrl":null,"url":null,"abstract":"<p><p>Neurosyphilis-induced dementia represents a severe manifestation of tertiary syphilis, characterized by cognitive and neuropsychiatric impairments. This condition arises from the progression of syphilis to the central nervous system, where the spirochete causes damage through invasion, chronic inflammation, and neurodegeneration. The pathophysiology involves chronic inflammatory responses, direct bacterial damage, and proteinopathies. <i>Treponema pallidum</i> triggers an inflammatory cascade, resulting in neuronal injury and synaptic dysfunction. Abnormal protein accumulations, including TAR DNA-binding protein 43 (TDP-43) and tau, contribute to neuronal loss and cognitive decline. Seizures, psychiatric symptoms, and motor deficits further complicate the progression of dementia. Diagnosis includes clinical assessment, cerebrospinal fluid analysis, and neuroimaging. Diagnostic tests include CSF-VDRL, FTA-ABS, and neuroimaging techniques such as MRI and PET scans, which help detect structural changes and confirm neurosyphilis. Management of neurosyphilis-induced dementia involves antibiotic therapy and psychotropic medications to address both infectious and symptomatic components. While penicillin remains the cornerstone of treatment, psychotropic agents, including haloperidol, risperidone, quetiapine, and divalproex sodium, can manage psychiatric symptoms. However, careful monitoring is required due to potential side effects and interactions with ongoing treatment. Overall, early diagnosis and comprehensive management are crucial for mitigating the cognitive and neuropsychiatric impairments associated with neurosyphilis-induced dementia.</p>","PeriodicalId":19130,"journal":{"name":"Neurology International","volume":"16 6","pages":"1653-1665"},"PeriodicalIF":3.3000,"publicationDate":"2024-12-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11679807/pdf/","citationCount":"0","resultStr":"{\"title\":\"Mechanisms of Neurosyphilis-Induced Dementia: Insights into Pathophysiology.\",\"authors\":\"Aya Fadel, Hussain Hussain, Robert J Hernandez, Amanda Marie Clichy Silva, Amir Agustin Estil-Las, Mohammad Hamad, Zahraa F Saadoon, Lamia Naseer, William C Sultan, Carla Sultan, Taylor Schnepp, Arumugam R Jayakumar\",\"doi\":\"10.3390/neurolint16060120\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Neurosyphilis-induced dementia represents a severe manifestation of tertiary syphilis, characterized by cognitive and neuropsychiatric impairments. This condition arises from the progression of syphilis to the central nervous system, where the spirochete causes damage through invasion, chronic inflammation, and neurodegeneration. The pathophysiology involves chronic inflammatory responses, direct bacterial damage, and proteinopathies. <i>Treponema pallidum</i> triggers an inflammatory cascade, resulting in neuronal injury and synaptic dysfunction. Abnormal protein accumulations, including TAR DNA-binding protein 43 (TDP-43) and tau, contribute to neuronal loss and cognitive decline. Seizures, psychiatric symptoms, and motor deficits further complicate the progression of dementia. Diagnosis includes clinical assessment, cerebrospinal fluid analysis, and neuroimaging. Diagnostic tests include CSF-VDRL, FTA-ABS, and neuroimaging techniques such as MRI and PET scans, which help detect structural changes and confirm neurosyphilis. Management of neurosyphilis-induced dementia involves antibiotic therapy and psychotropic medications to address both infectious and symptomatic components. While penicillin remains the cornerstone of treatment, psychotropic agents, including haloperidol, risperidone, quetiapine, and divalproex sodium, can manage psychiatric symptoms. However, careful monitoring is required due to potential side effects and interactions with ongoing treatment. Overall, early diagnosis and comprehensive management are crucial for mitigating the cognitive and neuropsychiatric impairments associated with neurosyphilis-induced dementia.</p>\",\"PeriodicalId\":19130,\"journal\":{\"name\":\"Neurology International\",\"volume\":\"16 6\",\"pages\":\"1653-1665\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2024-12-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11679807/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurology International\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/neurolint16060120\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/neurolint16060120","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Mechanisms of Neurosyphilis-Induced Dementia: Insights into Pathophysiology.
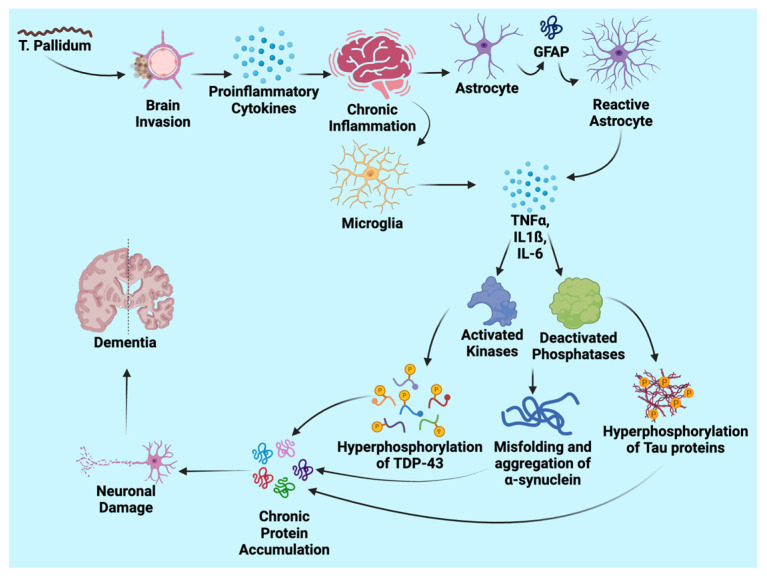
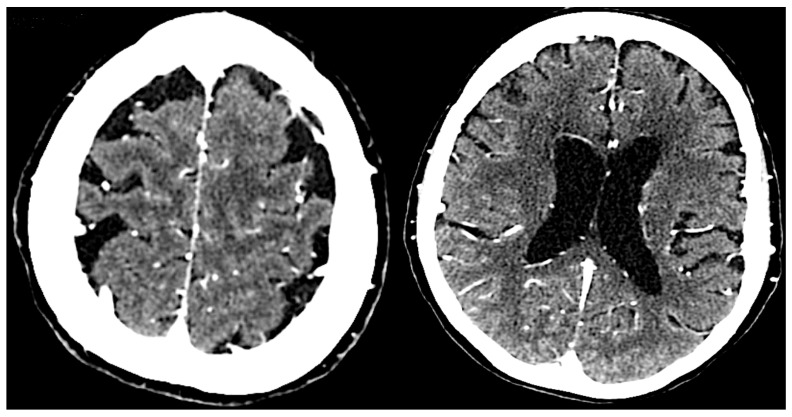
Neurosyphilis-induced dementia represents a severe manifestation of tertiary syphilis, characterized by cognitive and neuropsychiatric impairments. This condition arises from the progression of syphilis to the central nervous system, where the spirochete causes damage through invasion, chronic inflammation, and neurodegeneration. The pathophysiology involves chronic inflammatory responses, direct bacterial damage, and proteinopathies. Treponema pallidum triggers an inflammatory cascade, resulting in neuronal injury and synaptic dysfunction. Abnormal protein accumulations, including TAR DNA-binding protein 43 (TDP-43) and tau, contribute to neuronal loss and cognitive decline. Seizures, psychiatric symptoms, and motor deficits further complicate the progression of dementia. Diagnosis includes clinical assessment, cerebrospinal fluid analysis, and neuroimaging. Diagnostic tests include CSF-VDRL, FTA-ABS, and neuroimaging techniques such as MRI and PET scans, which help detect structural changes and confirm neurosyphilis. Management of neurosyphilis-induced dementia involves antibiotic therapy and psychotropic medications to address both infectious and symptomatic components. While penicillin remains the cornerstone of treatment, psychotropic agents, including haloperidol, risperidone, quetiapine, and divalproex sodium, can manage psychiatric symptoms. However, careful monitoring is required due to potential side effects and interactions with ongoing treatment. Overall, early diagnosis and comprehensive management are crucial for mitigating the cognitive and neuropsychiatric impairments associated with neurosyphilis-induced dementia.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
