Riccardo Cau, Francesco Pisu, Roberta Montisci, Tommaso D'Angelo, Cesare Mantini, Rodrigo Salgado, Luca Saba
{"title":"T1定位评估急性心包炎:一种支持性无造影剂CMR标记。","authors":"Riccardo Cau, Francesco Pisu, Roberta Montisci, Tommaso D'Angelo, Cesare Mantini, Rodrigo Salgado, Luca Saba","doi":"10.3390/tomography10120137","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The purpose of this study was to explore the impact of pericardial T1 mapping as a potential supportive non-contrast cardiovascular magnetic resonance (CMR) parameter in the diagnosis of acute pericarditis. Additionally, we investigated the relationship between T1 mapping values in acute pericarditis patients and their demographic data, cardiovascular risk factors, clinical parameters, cardiac biomarkers, and cardiac function.</p><p><strong>Method: </strong>This retrospective study included CMR scans in 35 consecutive patients with acute pericarditis (26 males, 45.54 ± 23.38 years). Moreover, we included 17 sex- and age-matched healthy controls (12 males, mean age 47.78 ±19.38 years). CMR-derived pericardial T1 mapping values, which included all pericardial structures within the pericardial layers-encompassing both pericardial effusion and pericardial layer thickness-were analyzed and compared between acute pericarditis patients and controls.</p><p><strong>Results: </strong>Compared to the matched control group, acute pericarditis patients demonstrated significantly lower pericardial T1 mapping values (2137 ms ± 519 vs. 3268 ms ± 362, <i>p</i> = 0.001). In the multivariable analysis, the pericardial T1 mapping value was independently associated with the severity of pericardial late gadolinium enhancement (LGE) (β coefficient = -3.271, <i>p</i> = 0.003). The receiver operating characteristic curve analysis showed that the diagnostic performance of pericardial T1 mapping in discriminating acute pericarditis patients was excellent, with an area under the curve of 0.97 (95% CI = 0.94-0.98), using a threshold of 2862.5 ms.</p><p><strong>Conclusions: </strong>Pericardial T1 mapping values could serve as an additional non-contrast CMR parameter for identifying patients with acute pericarditis, demonstrating an independent association with the severity of pericardial LGE.</p>","PeriodicalId":51330,"journal":{"name":"Tomography","volume":"10 12","pages":"1881-1894"},"PeriodicalIF":2.2000,"publicationDate":"2024-11-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11679063/pdf/","citationCount":"0","resultStr":"{\"title\":\"Assessing Acute Pericarditis with T1 Mapping: A Supportive Contrast-Free CMR Marker.\",\"authors\":\"Riccardo Cau, Francesco Pisu, Roberta Montisci, Tommaso D'Angelo, Cesare Mantini, Rodrigo Salgado, Luca Saba\",\"doi\":\"10.3390/tomography10120137\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The purpose of this study was to explore the impact of pericardial T1 mapping as a potential supportive non-contrast cardiovascular magnetic resonance (CMR) parameter in the diagnosis of acute pericarditis. Additionally, we investigated the relationship between T1 mapping values in acute pericarditis patients and their demographic data, cardiovascular risk factors, clinical parameters, cardiac biomarkers, and cardiac function.</p><p><strong>Method: </strong>This retrospective study included CMR scans in 35 consecutive patients with acute pericarditis (26 males, 45.54 ± 23.38 years). Moreover, we included 17 sex- and age-matched healthy controls (12 males, mean age 47.78 ±19.38 years). CMR-derived pericardial T1 mapping values, which included all pericardial structures within the pericardial layers-encompassing both pericardial effusion and pericardial layer thickness-were analyzed and compared between acute pericarditis patients and controls.</p><p><strong>Results: </strong>Compared to the matched control group, acute pericarditis patients demonstrated significantly lower pericardial T1 mapping values (2137 ms ± 519 vs. 3268 ms ± 362, <i>p</i> = 0.001). In the multivariable analysis, the pericardial T1 mapping value was independently associated with the severity of pericardial late gadolinium enhancement (LGE) (β coefficient = -3.271, <i>p</i> = 0.003). The receiver operating characteristic curve analysis showed that the diagnostic performance of pericardial T1 mapping in discriminating acute pericarditis patients was excellent, with an area under the curve of 0.97 (95% CI = 0.94-0.98), using a threshold of 2862.5 ms.</p><p><strong>Conclusions: </strong>Pericardial T1 mapping values could serve as an additional non-contrast CMR parameter for identifying patients with acute pericarditis, demonstrating an independent association with the severity of pericardial LGE.</p>\",\"PeriodicalId\":51330,\"journal\":{\"name\":\"Tomography\",\"volume\":\"10 12\",\"pages\":\"1881-1894\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2024-11-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11679063/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tomography\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3390/tomography10120137\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tomography","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3390/tomography10120137","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
摘要
目的:本研究的目的是探讨心包T1定位作为一种潜在的非对比心血管磁共振(CMR)辅助诊断急性心包炎的影响。此外,我们还研究了急性心包炎患者T1制图值与其人口学数据、心血管危险因素、临床参数、心脏生物标志物和心功能之间的关系。方法:回顾性研究连续35例急性心包炎患者(男性26例,45.54±23.38岁)的CMR扫描。此外,我们还纳入了17例性别和年龄匹配的健康对照(男性12例,平均年龄47.78±19.38岁)。我们分析并比较了急性心包炎患者和对照组的cmr心包T1测图值,其中包括心包层内的所有心包结构——包括心包积液和心包层厚度。结果:与对照组相比,急性心包炎患者心包T1测图值明显降低(2137 ms±519 vs. 3268 ms±362,p = 0.001)。在多变量分析中,心包T1测图值与心包晚期钆强化(LGE)严重程度独立相关(β系数= -3.271,p = 0.003)。受者工作特征曲线分析显示,心包T1测图对急性心包炎患者的诊断效果很好,曲线下面积为0.97 (95% CI = 0.94-0.98),阈值为2862.5 ms。结论:心包T1测图值可作为鉴别急性心包炎患者的额外非对比CMR参数,与心包LGE的严重程度独立相关。
Assessing Acute Pericarditis with T1 Mapping: A Supportive Contrast-Free CMR Marker.
Objective: The purpose of this study was to explore the impact of pericardial T1 mapping as a potential supportive non-contrast cardiovascular magnetic resonance (CMR) parameter in the diagnosis of acute pericarditis. Additionally, we investigated the relationship between T1 mapping values in acute pericarditis patients and their demographic data, cardiovascular risk factors, clinical parameters, cardiac biomarkers, and cardiac function.
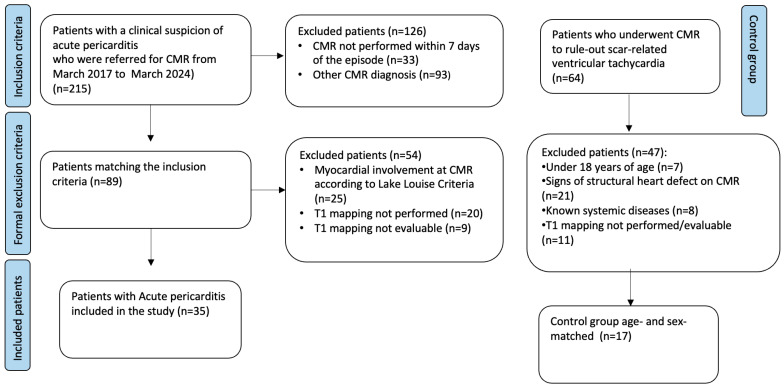
Method: This retrospective study included CMR scans in 35 consecutive patients with acute pericarditis (26 males, 45.54 ± 23.38 years). Moreover, we included 17 sex- and age-matched healthy controls (12 males, mean age 47.78 ±19.38 years). CMR-derived pericardial T1 mapping values, which included all pericardial structures within the pericardial layers-encompassing both pericardial effusion and pericardial layer thickness-were analyzed and compared between acute pericarditis patients and controls.
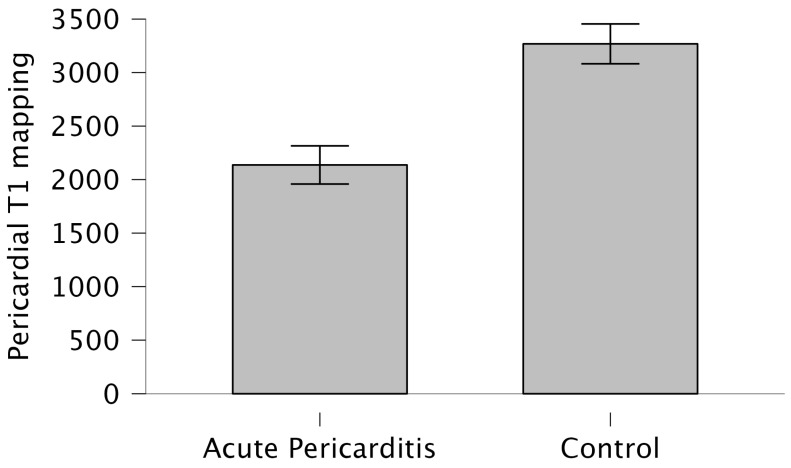
Results: Compared to the matched control group, acute pericarditis patients demonstrated significantly lower pericardial T1 mapping values (2137 ms ± 519 vs. 3268 ms ± 362, p = 0.001). In the multivariable analysis, the pericardial T1 mapping value was independently associated with the severity of pericardial late gadolinium enhancement (LGE) (β coefficient = -3.271, p = 0.003). The receiver operating characteristic curve analysis showed that the diagnostic performance of pericardial T1 mapping in discriminating acute pericarditis patients was excellent, with an area under the curve of 0.97 (95% CI = 0.94-0.98), using a threshold of 2862.5 ms.
Conclusions: Pericardial T1 mapping values could serve as an additional non-contrast CMR parameter for identifying patients with acute pericarditis, demonstrating an independent association with the severity of pericardial LGE.
TomographyMedicine-Radiology, Nuclear Medicine and Imaging
CiteScore
2.70
自引率
10.50%
发文量
222
期刊介绍:
TomographyTM publishes basic (technical and pre-clinical) and clinical scientific articles which involve the advancement of imaging technologies. Tomography encompasses studies that use single or multiple imaging modalities including for example CT, US, PET, SPECT, MR and hyperpolarization technologies, as well as optical modalities (i.e. bioluminescence, photoacoustic, endomicroscopy, fiber optic imaging and optical computed tomography) in basic sciences, engineering, preclinical and clinical medicine.
Tomography also welcomes studies involving exploration and refinement of contrast mechanisms and image-derived metrics within and across modalities toward the development of novel imaging probes for image-based feedback and intervention. The use of imaging in biology and medicine provides unparalleled opportunities to noninvasively interrogate tissues to obtain real-time dynamic and quantitative information required for diagnosis and response to interventions and to follow evolving pathological conditions. As multi-modal studies and the complexities of imaging technologies themselves are ever increasing to provide advanced information to scientists and clinicians.
Tomography provides a unique publication venue allowing investigators the opportunity to more precisely communicate integrated findings related to the diverse and heterogeneous features associated with underlying anatomical, physiological, functional, metabolic and molecular genetic activities of normal and diseased tissue. Thus Tomography publishes peer-reviewed articles which involve the broad use of imaging of any tissue and disease type including both preclinical and clinical investigations. In addition, hardware/software along with chemical and molecular probe advances are welcome as they are deemed to significantly contribute towards the long-term goal of improving the overall impact of imaging on scientific and clinical discovery.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
