{"title":"早期和晚期利妥昔单抗 BCD020 生物类似物对幼年系统性红斑狼疮 12 个月疗程的疗效:一项回顾性研究。","authors":"Elvira Kalashnikova, Eugenia Isupova, Ekaterina Gaidar, Natalia Lubimova, Lyubov Sorokina, Irina Chikova, Maria Kaneva, Rinat Raupov, Olga Kalashnikova, Damir Aliev, Inna Gaydukova, Mikhail Kostik","doi":"10.5527/wjn.v13.i4.98393","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Juvenile systemic lupus erythematosus (SLE) is a severe, life-threatening disease. However, the role of rituximab in managing juvenile SLE remains undefined, although early biological intervention may improve disease outcomes.</p><p><strong>Aim: </strong>To assess the differences in the outcomes of different types of rituximab administration (early and late).</p><p><strong>Methods: </strong>In this retrospective cohort study, the information of 36 children with SLE with early (less than 6 months from onset) rituximab administration (ERA), and late (more than 1 year) rituximab administration (LRA) was analyzed. We compared initial disease characteristics at onset, at baseline (start of rituximab), and at the end of the study (EOS) at 12 months, as well as outcomes and treatment characteristics.</p><p><strong>Results: </strong>The main differences at baseline were a higher daily median dose of corticosteroids, increased MAS frequency, and a higher Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) in the ERA group. No differences in the main SLE outcomes between groups at the EOS were observed. The part of lupus nephritis patients who achieved remission changed from 44% to 31% in ERA and 32% to 11% in the LRA group. Patients with ERA had a shorter time to achieve low daily corticosteroid dose (≤ 0.2 mg/kg) at 1.2 (0.9; 1.4) years compared to 2.8 (2.3; 4.0) years (<i>P</i> = 0.000001) and higher probability to achieve this low dose [hazard ratio (HR) = 57.8 (95% confidence interval (CI): 7.2-463.2), <i>P</i> = 0.00001 and remission (SLEDAI = 0); HR = 37.6 (95%CI: 4.45-333.3), <i>P</i> = 0.00001]. No differences in adverse events, including severe adverse events, were observed.</p><p><strong>Conclusion: </strong>ERA demonstrated a better steroid-sparing effect and a possibility of earlier remission or low disease activity, except for lupus nephritis. Further investigations are required.</p>","PeriodicalId":94272,"journal":{"name":"World journal of nephrology","volume":"13 4","pages":"98393"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11572657/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcomes of a 12-month course of early and late rituximab BCD020 biosimilar administration in juvenile systemic lupus erythematosus: A retrospective study.\",\"authors\":\"Elvira Kalashnikova, Eugenia Isupova, Ekaterina Gaidar, Natalia Lubimova, Lyubov Sorokina, Irina Chikova, Maria Kaneva, Rinat Raupov, Olga Kalashnikova, Damir Aliev, Inna Gaydukova, Mikhail Kostik\",\"doi\":\"10.5527/wjn.v13.i4.98393\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Juvenile systemic lupus erythematosus (SLE) is a severe, life-threatening disease. However, the role of rituximab in managing juvenile SLE remains undefined, although early biological intervention may improve disease outcomes.</p><p><strong>Aim: </strong>To assess the differences in the outcomes of different types of rituximab administration (early and late).</p><p><strong>Methods: </strong>In this retrospective cohort study, the information of 36 children with SLE with early (less than 6 months from onset) rituximab administration (ERA), and late (more than 1 year) rituximab administration (LRA) was analyzed. We compared initial disease characteristics at onset, at baseline (start of rituximab), and at the end of the study (EOS) at 12 months, as well as outcomes and treatment characteristics.</p><p><strong>Results: </strong>The main differences at baseline were a higher daily median dose of corticosteroids, increased MAS frequency, and a higher Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) in the ERA group. No differences in the main SLE outcomes between groups at the EOS were observed. The part of lupus nephritis patients who achieved remission changed from 44% to 31% in ERA and 32% to 11% in the LRA group. Patients with ERA had a shorter time to achieve low daily corticosteroid dose (≤ 0.2 mg/kg) at 1.2 (0.9; 1.4) years compared to 2.8 (2.3; 4.0) years (<i>P</i> = 0.000001) and higher probability to achieve this low dose [hazard ratio (HR) = 57.8 (95% confidence interval (CI): 7.2-463.2), <i>P</i> = 0.00001 and remission (SLEDAI = 0); HR = 37.6 (95%CI: 4.45-333.3), <i>P</i> = 0.00001]. No differences in adverse events, including severe adverse events, were observed.</p><p><strong>Conclusion: </strong>ERA demonstrated a better steroid-sparing effect and a possibility of earlier remission or low disease activity, except for lupus nephritis. Further investigations are required.</p>\",\"PeriodicalId\":94272,\"journal\":{\"name\":\"World journal of nephrology\",\"volume\":\"13 4\",\"pages\":\"98393\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-12-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11572657/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World journal of nephrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5527/wjn.v13.i4.98393\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World journal of nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5527/wjn.v13.i4.98393","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Outcomes of a 12-month course of early and late rituximab BCD020 biosimilar administration in juvenile systemic lupus erythematosus: A retrospective study.
Background: Juvenile systemic lupus erythematosus (SLE) is a severe, life-threatening disease. However, the role of rituximab in managing juvenile SLE remains undefined, although early biological intervention may improve disease outcomes.
Aim: To assess the differences in the outcomes of different types of rituximab administration (early and late).
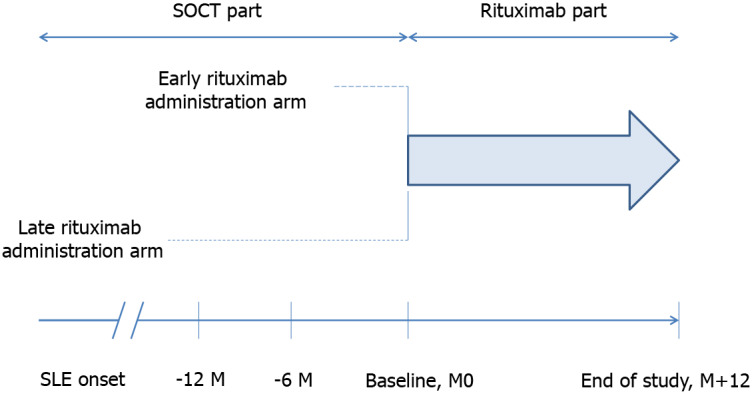
Methods: In this retrospective cohort study, the information of 36 children with SLE with early (less than 6 months from onset) rituximab administration (ERA), and late (more than 1 year) rituximab administration (LRA) was analyzed. We compared initial disease characteristics at onset, at baseline (start of rituximab), and at the end of the study (EOS) at 12 months, as well as outcomes and treatment characteristics.
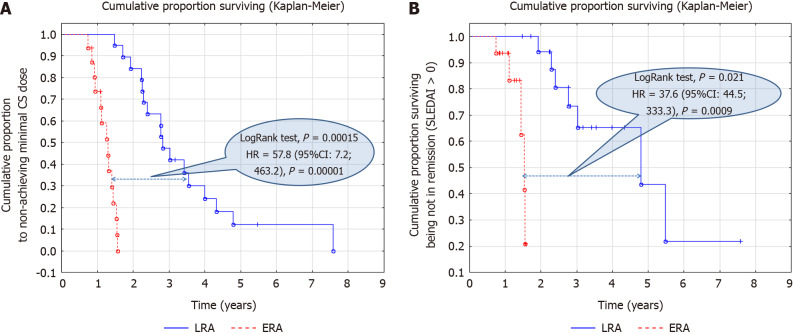
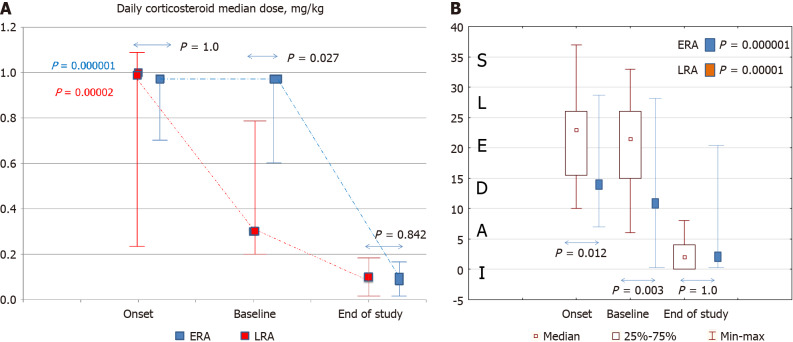
Results: The main differences at baseline were a higher daily median dose of corticosteroids, increased MAS frequency, and a higher Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) in the ERA group. No differences in the main SLE outcomes between groups at the EOS were observed. The part of lupus nephritis patients who achieved remission changed from 44% to 31% in ERA and 32% to 11% in the LRA group. Patients with ERA had a shorter time to achieve low daily corticosteroid dose (≤ 0.2 mg/kg) at 1.2 (0.9; 1.4) years compared to 2.8 (2.3; 4.0) years (P = 0.000001) and higher probability to achieve this low dose [hazard ratio (HR) = 57.8 (95% confidence interval (CI): 7.2-463.2), P = 0.00001 and remission (SLEDAI = 0); HR = 37.6 (95%CI: 4.45-333.3), P = 0.00001]. No differences in adverse events, including severe adverse events, were observed.
Conclusion: ERA demonstrated a better steroid-sparing effect and a possibility of earlier remission or low disease activity, except for lupus nephritis. Further investigations are required.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
