L Stewart Massad, Megan A Clarke, Rebecca B Perkins, Francisco Garcia, David Chelmow, Li C Cheung, Teresa M Darragh, Didem Egemen, Thomas S Lorey, Ritu Nayar, Morgan Newman, Carolann Risley, Robert A Smith, Nicolas Wentzensen
{"title":"应用扩展基因分型结果管理阳性宫颈阴道人乳头瘤病毒检测结果:持久的指南。","authors":"L Stewart Massad, Megan A Clarke, Rebecca B Perkins, Francisco Garcia, David Chelmow, Li C Cheung, Teresa M Darragh, Didem Egemen, Thomas S Lorey, Ritu Nayar, Morgan Newman, Carolann Risley, Robert A Smith, Nicolas Wentzensen","doi":"10.1097/LGT.0000000000000865","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The Enduring Consensus Cervical Cancer Screening and Management Guidelines Committee developed recommendations for the use of extended genotyping results in cervical cancer prevention programs.</p><p><strong>Methods: </strong>Risks of cervical intraepithelial neoplasia grade 3 or worse were calculated using data obtained with the Onclarity HPV Assay from large cohorts. Management recommendations were based on clinical action thresholds developed for the 2019 American Society for Colposcopy and Cervical Pathology Risk-Based Management Consensus Guidelines. Risk estimates were reviewed in relation to clinical action thresholds and used as the basis for draft recommendations. After an open comment period, recommendations were finalized and ratified through a vote by the Consensus Stakeholder Group.</p><p><strong>Results: </strong>Colposcopy is recommended after positive tests for human papillomavirus (HPV) types 16 and 18. For those positive for HPV 45, 33/58, 31, 52, 35/39/68, or 51 but negative for 16 or 18, triage with cytology or dual stain testing is recommended. When screening with primary HPV testing, for patients who test positive for HPV types 56/59/66 and no other carcinogenic types, repeat HPV testing in 1 year is recommended. When screening with cotesting, for those who test positive for HPV types 56/59/66 and no other carcinogenic types, 1-year return is recommended for negative for intraepithelial lesion or malignancy, atypical squamous cells of undetermined significance, and low-grade squamous intraepithelial lesion, and colposcopy is recommended for atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion (ASC-H), atypical glandular cells, high-grade squamous intraepithelial lesion, or carcinoma. When patients without prior high-grade cytology (atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion, atypical glandular cells, high-grade squamous intraepithelial lesion, or carcinoma) or histology (cervical intraepithelial neoplasia [CIN]2, CIN3, or adenocarcinoma in situ) are being followed, use of extended genotyping results is acceptable. When high-grade cytology or histology results are present, or when patients are being followed after treatment of CIN2+, management using the 2019 guidelines is recommended.</p><p><strong>Conclusions: </strong>Human papillomavirus extended genotyping can guide clinical management in the setting of a positive HPV test result.</p>","PeriodicalId":50160,"journal":{"name":"Journal of Lower Genital Tract Disease","volume":" ","pages":"134-143"},"PeriodicalIF":2.1000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11939109/pdf/","citationCount":"0","resultStr":"{\"title\":\"Applying Results of Extended Genotyping to Management of Positive Cervicovaginal Human Papillomavirus Test Results: Enduring Guidelines.\",\"authors\":\"L Stewart Massad, Megan A Clarke, Rebecca B Perkins, Francisco Garcia, David Chelmow, Li C Cheung, Teresa M Darragh, Didem Egemen, Thomas S Lorey, Ritu Nayar, Morgan Newman, Carolann Risley, Robert A Smith, Nicolas Wentzensen\",\"doi\":\"10.1097/LGT.0000000000000865\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The Enduring Consensus Cervical Cancer Screening and Management Guidelines Committee developed recommendations for the use of extended genotyping results in cervical cancer prevention programs.</p><p><strong>Methods: </strong>Risks of cervical intraepithelial neoplasia grade 3 or worse were calculated using data obtained with the Onclarity HPV Assay from large cohorts. Management recommendations were based on clinical action thresholds developed for the 2019 American Society for Colposcopy and Cervical Pathology Risk-Based Management Consensus Guidelines. Risk estimates were reviewed in relation to clinical action thresholds and used as the basis for draft recommendations. After an open comment period, recommendations were finalized and ratified through a vote by the Consensus Stakeholder Group.</p><p><strong>Results: </strong>Colposcopy is recommended after positive tests for human papillomavirus (HPV) types 16 and 18. For those positive for HPV 45, 33/58, 31, 52, 35/39/68, or 51 but negative for 16 or 18, triage with cytology or dual stain testing is recommended. When screening with primary HPV testing, for patients who test positive for HPV types 56/59/66 and no other carcinogenic types, repeat HPV testing in 1 year is recommended. When screening with cotesting, for those who test positive for HPV types 56/59/66 and no other carcinogenic types, 1-year return is recommended for negative for intraepithelial lesion or malignancy, atypical squamous cells of undetermined significance, and low-grade squamous intraepithelial lesion, and colposcopy is recommended for atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion (ASC-H), atypical glandular cells, high-grade squamous intraepithelial lesion, or carcinoma. When patients without prior high-grade cytology (atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion, atypical glandular cells, high-grade squamous intraepithelial lesion, or carcinoma) or histology (cervical intraepithelial neoplasia [CIN]2, CIN3, or adenocarcinoma in situ) are being followed, use of extended genotyping results is acceptable. When high-grade cytology or histology results are present, or when patients are being followed after treatment of CIN2+, management using the 2019 guidelines is recommended.</p><p><strong>Conclusions: </strong>Human papillomavirus extended genotyping can guide clinical management in the setting of a positive HPV test result.</p>\",\"PeriodicalId\":50160,\"journal\":{\"name\":\"Journal of Lower Genital Tract Disease\",\"volume\":\" \",\"pages\":\"134-143\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11939109/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Lower Genital Tract Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/LGT.0000000000000865\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Lower Genital Tract Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/LGT.0000000000000865","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Applying Results of Extended Genotyping to Management of Positive Cervicovaginal Human Papillomavirus Test Results: Enduring Guidelines.
Objective: The Enduring Consensus Cervical Cancer Screening and Management Guidelines Committee developed recommendations for the use of extended genotyping results in cervical cancer prevention programs.
Methods: Risks of cervical intraepithelial neoplasia grade 3 or worse were calculated using data obtained with the Onclarity HPV Assay from large cohorts. Management recommendations were based on clinical action thresholds developed for the 2019 American Society for Colposcopy and Cervical Pathology Risk-Based Management Consensus Guidelines. Risk estimates were reviewed in relation to clinical action thresholds and used as the basis for draft recommendations. After an open comment period, recommendations were finalized and ratified through a vote by the Consensus Stakeholder Group.
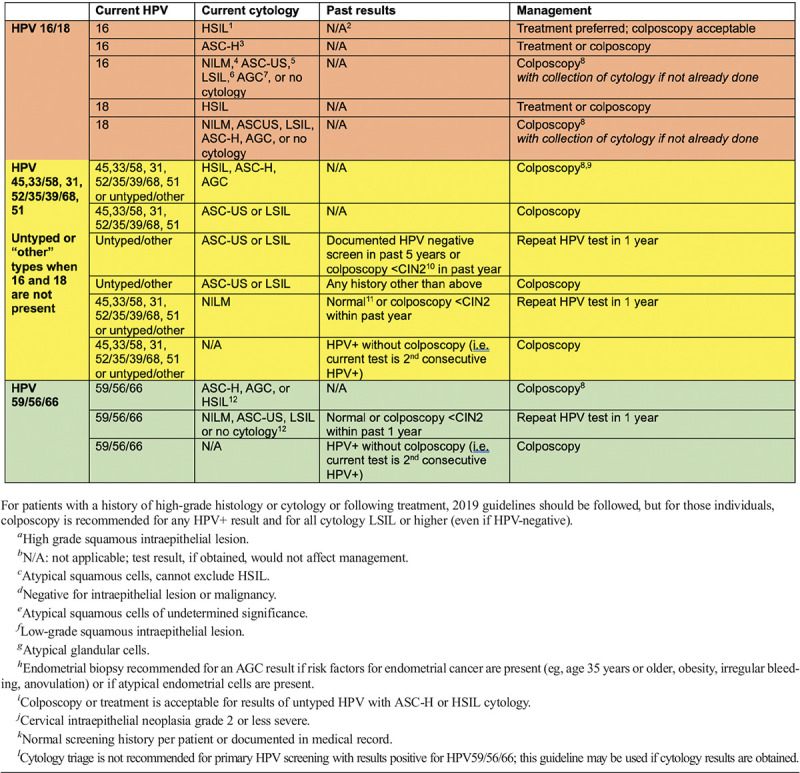
Results: Colposcopy is recommended after positive tests for human papillomavirus (HPV) types 16 and 18. For those positive for HPV 45, 33/58, 31, 52, 35/39/68, or 51 but negative for 16 or 18, triage with cytology or dual stain testing is recommended. When screening with primary HPV testing, for patients who test positive for HPV types 56/59/66 and no other carcinogenic types, repeat HPV testing in 1 year is recommended. When screening with cotesting, for those who test positive for HPV types 56/59/66 and no other carcinogenic types, 1-year return is recommended for negative for intraepithelial lesion or malignancy, atypical squamous cells of undetermined significance, and low-grade squamous intraepithelial lesion, and colposcopy is recommended for atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion (ASC-H), atypical glandular cells, high-grade squamous intraepithelial lesion, or carcinoma. When patients without prior high-grade cytology (atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion, atypical glandular cells, high-grade squamous intraepithelial lesion, or carcinoma) or histology (cervical intraepithelial neoplasia [CIN]2, CIN3, or adenocarcinoma in situ) are being followed, use of extended genotyping results is acceptable. When high-grade cytology or histology results are present, or when patients are being followed after treatment of CIN2+, management using the 2019 guidelines is recommended.
Conclusions: Human papillomavirus extended genotyping can guide clinical management in the setting of a positive HPV test result.
期刊介绍:
The Journal of Lower Genital Tract Disease is the source for the latest science about benign and malignant conditions of the cervix, vagina, vulva, and anus.
The Journal publishes peer-reviewed original research original research that addresses prevalence, causes, mechanisms, diagnosis, course, treatment, and prevention of lower genital tract disease. We publish clinical guidelines, position papers, cost-effectiveness analyses, narrative reviews, and systematic reviews, including meta-analyses. We also publish papers about research and reporting methods, opinions about controversial medical issues. Of particular note, we encourage material in any of the above mentioned categories that is related to improving patient care, avoiding medical errors, and comparative effectiveness research. We encourage publication of evidence-based guidelines, diagnostic and therapeutic algorithms, and decision aids. Original research and reviews may be sub-classified according to topic: cervix and HPV, vulva and vagina, perianal and anal, basic science, and education and learning.
The scope and readership of the journal extend to several disciplines: gynecology, internal medicine, family practice, dermatology, physical therapy, pathology, sociology, psychology, anthropology, sex therapy, and pharmacology. The Journal of Lower Genital Tract Disease highlights needs for future research, and enhances health care.
The Journal of Lower Genital Tract Disease is the official journal of the American Society for Colposcopy and Cervical Pathology, the International Society for the Study of Vulvovaginal Disease, and the International Federation of Cervical Pathology and Colposcopy, and sponsored by the Australian Society for Colposcopy and Cervical Pathology and the Society of Canadian Colposcopists.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
