Kyle W. Blackburn BS , Susan Y. Green MPH , Allen Kuncheria BA , Meng Li PhD , Adel M. Hassan BA , Brittany Rhoades PhD , Scott A. Weldon MA , Subhasis Chatterjee MD , Marc R. Moon MD , Scott A. LeMaire MD , Joseph S. Coselli MD
{"title":"预测择期胸腹主动脉瘤开放性修复患者的手术死亡率。","authors":"Kyle W. Blackburn BS , Susan Y. Green MPH , Allen Kuncheria BA , Meng Li PhD , Adel M. Hassan BA , Brittany Rhoades PhD , Scott A. Weldon MA , Subhasis Chatterjee MD , Marc R. Moon MD , Scott A. LeMaire MD , Joseph S. Coselli MD","doi":"10.1016/j.xjon.2024.09.002","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>We have developed a model aimed at identifying preoperative predictors of operative mortality in patients who undergo elective, open thoracoabdominal aortic aneurysm (TAAA) repair. We converted this model into an intuitive nomogram to aid preoperative counseling.</div></div><div><h3>Methods</h3><div>We retrospectively analyzed data from 2884 elective, open TAAA repairs performed between 1986 and 2023 in a single practice. Using clinical and selected operative variables, we built 4 predictive models: multivariable logistic regression (MLR), random forest, support vector machine, and gradient boosting machine. Each model’s predictive effectiveness was evaluated with the C-statistic. Test C-statistics were computed using an 80:20 cross-validation scheme with 1000 iterations.</div></div><div><h3>Results</h3><div>Operative death occurred in 200 patients (6.9%). Test set C-statistics showed that the MLR model (median, 0.68; interquartile range [IQR], 0.65-0.71) outperformed the machine learning models (0.61 [IQR, 0.59-0.64] for random forest; 0.61 [IQR, 0.58-0.64] for support vector machine; 0.65 [IQR, 0.62-0.67] for gradient boosting machine). The final MLR model was based on 7 characteristics: increasing age (odds ratio [OR], 1.04/y; <em>P</em> < .001), cerebrovascular disease (OR, 1.54; <em>P</em> = .01), chronic kidney disease (OR, 1.53; <em>P</em> = .008), symptomatic aneurysm (OR, 1.42; <em>P</em> = .02), and Crawford extent I (OR, 0.66; <em>P</em> = .08), extent II (OR, 1.61; <em>P</em> = .01), and extent IV (OR, 0.41; <em>P</em> = .002). We converted this model into a nomogram.</div></div><div><h3>Conclusions</h3><div>Using institutional data, we evaluated several models to predict operative mortality in elective TAAA repair, using information available to surgeons preoperatively. We then converted the best predictive model, the MLR model, into an intuitive nomogram to aid patient counseling.</div></div>","PeriodicalId":74032,"journal":{"name":"JTCVS open","volume":"22 ","pages":"Pages 95-103"},"PeriodicalIF":1.9000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11704537/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predicting operative mortality in patients who undergo elective open thoracoabdominal aortic aneurysm repair\",\"authors\":\"Kyle W. Blackburn BS , Susan Y. Green MPH , Allen Kuncheria BA , Meng Li PhD , Adel M. Hassan BA , Brittany Rhoades PhD , Scott A. Weldon MA , Subhasis Chatterjee MD , Marc R. Moon MD , Scott A. LeMaire MD , Joseph S. Coselli MD\",\"doi\":\"10.1016/j.xjon.2024.09.002\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><div>We have developed a model aimed at identifying preoperative predictors of operative mortality in patients who undergo elective, open thoracoabdominal aortic aneurysm (TAAA) repair. We converted this model into an intuitive nomogram to aid preoperative counseling.</div></div><div><h3>Methods</h3><div>We retrospectively analyzed data from 2884 elective, open TAAA repairs performed between 1986 and 2023 in a single practice. Using clinical and selected operative variables, we built 4 predictive models: multivariable logistic regression (MLR), random forest, support vector machine, and gradient boosting machine. Each model’s predictive effectiveness was evaluated with the C-statistic. Test C-statistics were computed using an 80:20 cross-validation scheme with 1000 iterations.</div></div><div><h3>Results</h3><div>Operative death occurred in 200 patients (6.9%). Test set C-statistics showed that the MLR model (median, 0.68; interquartile range [IQR], 0.65-0.71) outperformed the machine learning models (0.61 [IQR, 0.59-0.64] for random forest; 0.61 [IQR, 0.58-0.64] for support vector machine; 0.65 [IQR, 0.62-0.67] for gradient boosting machine). The final MLR model was based on 7 characteristics: increasing age (odds ratio [OR], 1.04/y; <em>P</em> < .001), cerebrovascular disease (OR, 1.54; <em>P</em> = .01), chronic kidney disease (OR, 1.53; <em>P</em> = .008), symptomatic aneurysm (OR, 1.42; <em>P</em> = .02), and Crawford extent I (OR, 0.66; <em>P</em> = .08), extent II (OR, 1.61; <em>P</em> = .01), and extent IV (OR, 0.41; <em>P</em> = .002). We converted this model into a nomogram.</div></div><div><h3>Conclusions</h3><div>Using institutional data, we evaluated several models to predict operative mortality in elective TAAA repair, using information available to surgeons preoperatively. We then converted the best predictive model, the MLR model, into an intuitive nomogram to aid patient counseling.</div></div>\",\"PeriodicalId\":74032,\"journal\":{\"name\":\"JTCVS open\",\"volume\":\"22 \",\"pages\":\"Pages 95-103\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11704537/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JTCVS open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S266627362400250X\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTCVS open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S266627362400250X","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/10 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Predicting operative mortality in patients who undergo elective open thoracoabdominal aortic aneurysm repair
Background
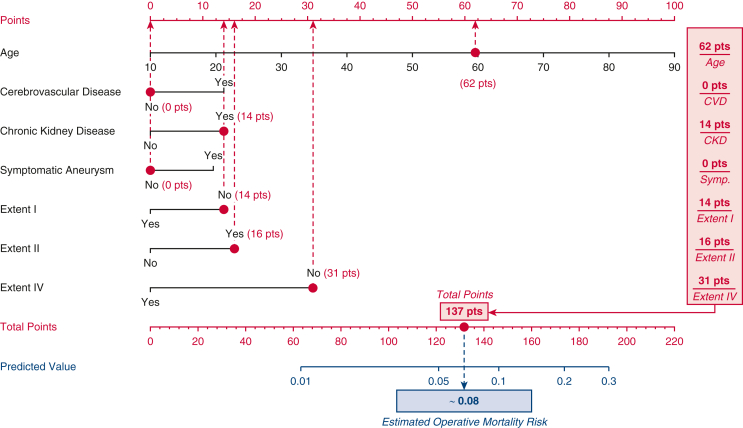
We have developed a model aimed at identifying preoperative predictors of operative mortality in patients who undergo elective, open thoracoabdominal aortic aneurysm (TAAA) repair. We converted this model into an intuitive nomogram to aid preoperative counseling.
Methods
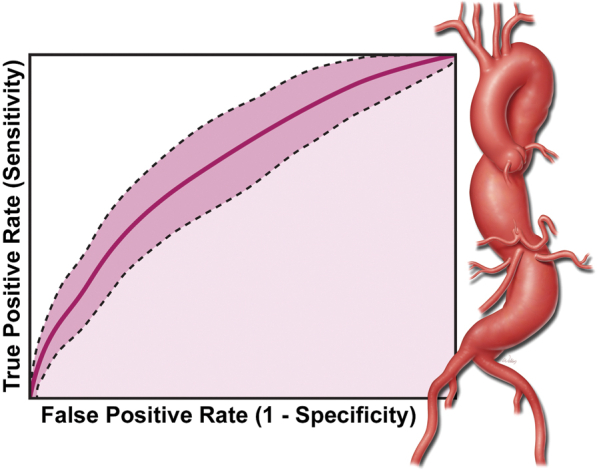
We retrospectively analyzed data from 2884 elective, open TAAA repairs performed between 1986 and 2023 in a single practice. Using clinical and selected operative variables, we built 4 predictive models: multivariable logistic regression (MLR), random forest, support vector machine, and gradient boosting machine. Each model’s predictive effectiveness was evaluated with the C-statistic. Test C-statistics were computed using an 80:20 cross-validation scheme with 1000 iterations.
Results
Operative death occurred in 200 patients (6.9%). Test set C-statistics showed that the MLR model (median, 0.68; interquartile range [IQR], 0.65-0.71) outperformed the machine learning models (0.61 [IQR, 0.59-0.64] for random forest; 0.61 [IQR, 0.58-0.64] for support vector machine; 0.65 [IQR, 0.62-0.67] for gradient boosting machine). The final MLR model was based on 7 characteristics: increasing age (odds ratio [OR], 1.04/y; P < .001), cerebrovascular disease (OR, 1.54; P = .01), chronic kidney disease (OR, 1.53; P = .008), symptomatic aneurysm (OR, 1.42; P = .02), and Crawford extent I (OR, 0.66; P = .08), extent II (OR, 1.61; P = .01), and extent IV (OR, 0.41; P = .002). We converted this model into a nomogram.
Conclusions
Using institutional data, we evaluated several models to predict operative mortality in elective TAAA repair, using information available to surgeons preoperatively. We then converted the best predictive model, the MLR model, into an intuitive nomogram to aid patient counseling.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
