{"title":"右美托咪定与芬太尼全静脉麻醉技术对急诊开颅急性外伤性硬膜下血肿患者异丙酚需求、脑松弛、颅内压、神经元损伤和血流动力学参数的比较:一项随机对照试验。","authors":"Vivek Chandar Chinnarasan, Prasanna Udupi Bidkar, Srinivasan Swaminathan, Manoranjitha Mani, Balasubramaniyan Vairappan, Protiti Chatterjee, Jerry Jame Joy, Ankita Dey, Rajasekar Ramadurai, Adethen Gunasekaran","doi":"10.25259/SNI_892_2024","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Propofol is one of the most used intravenous anesthetic agents in traumatic brain injury (TBI) patients undergoing emergency neurosurgical procedures. Despite being efficacious, its administration is associated with dose-related adverse effects. The use of adjuvants along with propofol aids in limiting its consumption, thereby mitigating the side effects related to propofol usage. This study aims to compare the safety and efficacy of dexmedetomidine-propofol versus fentanyl-propofol-based total intravenous anesthesia (TIVA) in adult TBI patients.</p><p><strong>Methods: </strong>A hundred patients posted for emergency evacuation of acute subdural hematoma were enrolled, and they were randomized into two groups of 50 each. Propofol-based TIVA with a Schneider target-controlled infusion model was used for induction and maintenance. Patients in Group F received fentanyl, and those in Group D received dexmedetomidine infusions as adjuvants. Advanced hemodynamic parameters were monitored. Intracranial pressure (ICP) and brain relaxation were measured after dural opening. The mean propofol consumption, number of additional fentanyl boluses, and blood samples for S100b (a biomarker of neuronal injury) were also collected.</p><p><strong>Results: </strong>The mean propofol consumption in Group D (88.7 ± 31.8 μg/kg/min) was lower when compared to Group F (107.9 ± 34.6 μg/kg/min), (<i>P</i> = 0.005). The mean intraoperative fentanyl requirement and postoperative S100b were significantly reduced in Group D. Subdural ICPs and brain relaxation scores were comparable. Hemodynamic parameters were well maintained in both groups.</p><p><strong>Conclusion: </strong>In TBI, dexmedetomidine as an adjunct to propofol-based TIVA results in a greater reduction in total propofol consumption and intraoperative opioid requirements while maintaining hemodynamic stability when compared to fentanyl.</p>","PeriodicalId":94217,"journal":{"name":"Surgical neurology international","volume":"15 ","pages":"462"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11704446/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of dexmedetomidine versus fentanyl-based total intravenous anesthesia technique on the requirement of propofol, brain relaxation, intracranial pressure, neuronal injury, and hemodynamic parameters in patients with acute traumatic subdural hematoma undergoing emergency craniotomy: A randomized controlled trial.\",\"authors\":\"Vivek Chandar Chinnarasan, Prasanna Udupi Bidkar, Srinivasan Swaminathan, Manoranjitha Mani, Balasubramaniyan Vairappan, Protiti Chatterjee, Jerry Jame Joy, Ankita Dey, Rajasekar Ramadurai, Adethen Gunasekaran\",\"doi\":\"10.25259/SNI_892_2024\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Propofol is one of the most used intravenous anesthetic agents in traumatic brain injury (TBI) patients undergoing emergency neurosurgical procedures. Despite being efficacious, its administration is associated with dose-related adverse effects. The use of adjuvants along with propofol aids in limiting its consumption, thereby mitigating the side effects related to propofol usage. This study aims to compare the safety and efficacy of dexmedetomidine-propofol versus fentanyl-propofol-based total intravenous anesthesia (TIVA) in adult TBI patients.</p><p><strong>Methods: </strong>A hundred patients posted for emergency evacuation of acute subdural hematoma were enrolled, and they were randomized into two groups of 50 each. Propofol-based TIVA with a Schneider target-controlled infusion model was used for induction and maintenance. Patients in Group F received fentanyl, and those in Group D received dexmedetomidine infusions as adjuvants. Advanced hemodynamic parameters were monitored. Intracranial pressure (ICP) and brain relaxation were measured after dural opening. The mean propofol consumption, number of additional fentanyl boluses, and blood samples for S100b (a biomarker of neuronal injury) were also collected.</p><p><strong>Results: </strong>The mean propofol consumption in Group D (88.7 ± 31.8 μg/kg/min) was lower when compared to Group F (107.9 ± 34.6 μg/kg/min), (<i>P</i> = 0.005). The mean intraoperative fentanyl requirement and postoperative S100b were significantly reduced in Group D. Subdural ICPs and brain relaxation scores were comparable. Hemodynamic parameters were well maintained in both groups.</p><p><strong>Conclusion: </strong>In TBI, dexmedetomidine as an adjunct to propofol-based TIVA results in a greater reduction in total propofol consumption and intraoperative opioid requirements while maintaining hemodynamic stability when compared to fentanyl.</p>\",\"PeriodicalId\":94217,\"journal\":{\"name\":\"Surgical neurology international\",\"volume\":\"15 \",\"pages\":\"462\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-12-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11704446/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical neurology international\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.25259/SNI_892_2024\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical neurology international","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25259/SNI_892_2024","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Comparison of dexmedetomidine versus fentanyl-based total intravenous anesthesia technique on the requirement of propofol, brain relaxation, intracranial pressure, neuronal injury, and hemodynamic parameters in patients with acute traumatic subdural hematoma undergoing emergency craniotomy: A randomized controlled trial.
Background: Propofol is one of the most used intravenous anesthetic agents in traumatic brain injury (TBI) patients undergoing emergency neurosurgical procedures. Despite being efficacious, its administration is associated with dose-related adverse effects. The use of adjuvants along with propofol aids in limiting its consumption, thereby mitigating the side effects related to propofol usage. This study aims to compare the safety and efficacy of dexmedetomidine-propofol versus fentanyl-propofol-based total intravenous anesthesia (TIVA) in adult TBI patients.
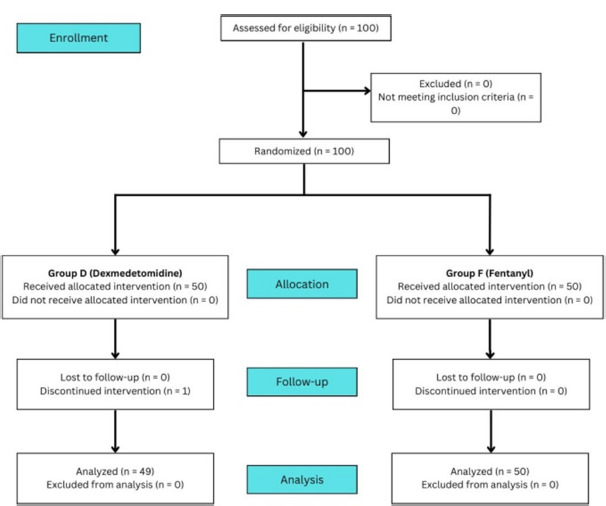
Methods: A hundred patients posted for emergency evacuation of acute subdural hematoma were enrolled, and they were randomized into two groups of 50 each. Propofol-based TIVA with a Schneider target-controlled infusion model was used for induction and maintenance. Patients in Group F received fentanyl, and those in Group D received dexmedetomidine infusions as adjuvants. Advanced hemodynamic parameters were monitored. Intracranial pressure (ICP) and brain relaxation were measured after dural opening. The mean propofol consumption, number of additional fentanyl boluses, and blood samples for S100b (a biomarker of neuronal injury) were also collected.
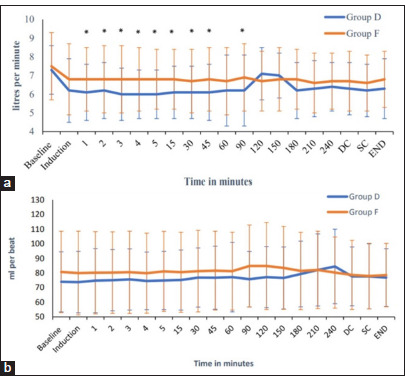
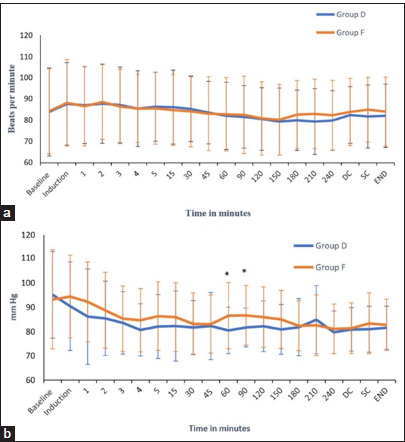
Results: The mean propofol consumption in Group D (88.7 ± 31.8 μg/kg/min) was lower when compared to Group F (107.9 ± 34.6 μg/kg/min), (P = 0.005). The mean intraoperative fentanyl requirement and postoperative S100b were significantly reduced in Group D. Subdural ICPs and brain relaxation scores were comparable. Hemodynamic parameters were well maintained in both groups.
Conclusion: In TBI, dexmedetomidine as an adjunct to propofol-based TIVA results in a greater reduction in total propofol consumption and intraoperative opioid requirements while maintaining hemodynamic stability when compared to fentanyl.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
