Brian K. Mitchell MD , Anna Tomdio MD , Muhammad S. Pir MD , Suraj K. Mishra MD , Pradeep Dayanand MD , Guillaume Bonnet MD, PhD , Maria C. Alu MS , Zachary M. Gertz MD
{"title":"一项空腹与自由口服心导管插入术的随机试验:CALORI试验。","authors":"Brian K. Mitchell MD , Anna Tomdio MD , Muhammad S. Pir MD , Suraj K. Mishra MD , Pradeep Dayanand MD , Guillaume Bonnet MD, PhD , Maria C. Alu MS , Zachary M. Gertz MD","doi":"10.1016/j.jscai.2024.102291","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Routine preprocedural fasting before cardiac catheterization remains common practice, despite a lack of robust evidence to support this practice. We investigated the impact of a liberal nonfasting strategy vs a standardized nil per os (NPO) regimen prior to cardiac catheterization.</div></div><div><h3>Methods</h3><div>Adult inpatients undergoing elective or urgent cardiac catheterization were randomized (1:1 ratio) to either NPO past midnight or ad libitum intake of liquids and solids (without dietary constraints) until immediately prior to the procedure. Only patients at high risk of aspiration or undergoing complex interventions were excluded. The primary end point was preprocedural patient-reported well-being scores (scaled 0-5, with 0 signifying absence of ailment and 5 the most extreme form), for variables including hunger, fatigue, anxiety, and nausea. A composite score summed the individual scores for hunger and fatigue. Other end points were periprocedural adverse events including emesis, aspiration, or intubation, in addition to postprocedural satisfaction.</div></div><div><h3>Results</h3><div>A total of 198 patients (65% male and 42% Black) were included in the final analysis. There were no differences in baseline characteristics between groups. Time from most recent oral intake (liquid or solid) to the start of the procedure averaged 148 minutes for the nonfasting group and 970 minutes for the NPO strategy (<em>P</em> < .001). The composite preprocedural well-being score was significantly better in the nonfasting arm (2.4 ± 2.4 nonfasting vs 6.0 ± 2.5 NPO; <em>P</em> < .001), as were the individual components of hunger (0.9 ± 1.5 vs 3.7 ± 1.5; <em>P</em> < .001), fatigue (1.5 ± 1.6 vs 2.3 ± 1.8; <em>P</em> < .001), and nausea (0.1 ± 0.5 vs 0.5 ±1.2; <em>P</em> = .006). There were no significant differences in adverse events between groups. Overall postprocedural satisfaction scores were significantly better in the nonfasting vs NPO group (0.3 ± 0.7 vs 1.0 ± 1.3, respectively; <em>P</em> < .001).</div></div><div><h3>Conclusions</h3><div>In this single-center randomized trial, a liberal nonfasting strategy prior to cardiac catheterization significantly improved patient well-being and satisfaction without compromising safety. Given the findings of this and other studies, routine fasting prior to cardiac catheterization should be reconsidered.</div></div>","PeriodicalId":73990,"journal":{"name":"Journal of the Society for Cardiovascular Angiography & Interventions","volume":"3 12","pages":"Article 102291"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11725108/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Randomized Trial of Cardiac Catheterization With Fasting Versus Liberal Oral Intake: The CALORI Trial\",\"authors\":\"Brian K. Mitchell MD , Anna Tomdio MD , Muhammad S. Pir MD , Suraj K. Mishra MD , Pradeep Dayanand MD , Guillaume Bonnet MD, PhD , Maria C. Alu MS , Zachary M. Gertz MD\",\"doi\":\"10.1016/j.jscai.2024.102291\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><div>Routine preprocedural fasting before cardiac catheterization remains common practice, despite a lack of robust evidence to support this practice. We investigated the impact of a liberal nonfasting strategy vs a standardized nil per os (NPO) regimen prior to cardiac catheterization.</div></div><div><h3>Methods</h3><div>Adult inpatients undergoing elective or urgent cardiac catheterization were randomized (1:1 ratio) to either NPO past midnight or ad libitum intake of liquids and solids (without dietary constraints) until immediately prior to the procedure. Only patients at high risk of aspiration or undergoing complex interventions were excluded. The primary end point was preprocedural patient-reported well-being scores (scaled 0-5, with 0 signifying absence of ailment and 5 the most extreme form), for variables including hunger, fatigue, anxiety, and nausea. A composite score summed the individual scores for hunger and fatigue. Other end points were periprocedural adverse events including emesis, aspiration, or intubation, in addition to postprocedural satisfaction.</div></div><div><h3>Results</h3><div>A total of 198 patients (65% male and 42% Black) were included in the final analysis. There were no differences in baseline characteristics between groups. Time from most recent oral intake (liquid or solid) to the start of the procedure averaged 148 minutes for the nonfasting group and 970 minutes for the NPO strategy (<em>P</em> < .001). The composite preprocedural well-being score was significantly better in the nonfasting arm (2.4 ± 2.4 nonfasting vs 6.0 ± 2.5 NPO; <em>P</em> < .001), as were the individual components of hunger (0.9 ± 1.5 vs 3.7 ± 1.5; <em>P</em> < .001), fatigue (1.5 ± 1.6 vs 2.3 ± 1.8; <em>P</em> < .001), and nausea (0.1 ± 0.5 vs 0.5 ±1.2; <em>P</em> = .006). There were no significant differences in adverse events between groups. Overall postprocedural satisfaction scores were significantly better in the nonfasting vs NPO group (0.3 ± 0.7 vs 1.0 ± 1.3, respectively; <em>P</em> < .001).</div></div><div><h3>Conclusions</h3><div>In this single-center randomized trial, a liberal nonfasting strategy prior to cardiac catheterization significantly improved patient well-being and satisfaction without compromising safety. Given the findings of this and other studies, routine fasting prior to cardiac catheterization should be reconsidered.</div></div>\",\"PeriodicalId\":73990,\"journal\":{\"name\":\"Journal of the Society for Cardiovascular Angiography & Interventions\",\"volume\":\"3 12\",\"pages\":\"Article 102291\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11725108/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Society for Cardiovascular Angiography & Interventions\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2772930324017356\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Society for Cardiovascular Angiography & Interventions","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2772930324017356","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:尽管缺乏强有力的证据支持,心导管插入术前的常规术前禁食仍然是一种常见的做法。我们研究了在心导管插入术前自由非禁食策略与标准化零氧(NPO)方案的影响。方法:接受选择性或紧急心导管插入术的成年住院患者被随机(1:1比例)分为两组,一组在午夜过后进食,另一组在手术前随意进食液体和固体(没有饮食限制)。仅排除吸入风险高或正在接受复杂干预的患者。主要终点是手术前患者报告的幸福感评分(0-5分,0表示没有疾病,5表示最极端的形式),变量包括饥饿、疲劳、焦虑和恶心。一个综合分数综合了个人在饥饿和疲劳方面的得分。其他终点是围手术期不良事件,包括呕吐、误吸或插管,以及术后满意度。结果:198例患者(男性65%,黑人42%)纳入最终分析。两组间基线特征无差异。非禁食组从最近一次口服(液体或固体)到手术开始的平均时间为148分钟,NPO组为970分钟(P < 0.001)。非禁食组的综合手术前幸福感评分显著高于非禁食组(2.4±2.4 NPO vs 6.0±2.5 NPO);P < 0.001),饥饿的各个成分也是如此(0.9±1.5 vs 3.7±1.5;P < 0.001),疲劳(1.5±1.6 vs 2.3±1.8;P < 0.001),恶心(0.1±0.5 vs 0.5±1.2;P = .006)。两组间不良事件发生率无显著差异。非禁食组和NPO组的总体术后满意度得分显著高于对照组(分别为0.3±0.7和1.0±1.3);P < 0.001)。结论:在这项单中心随机试验中,心导管插入术前的自由非禁食策略显著提高了患者的幸福感和满意度,同时不影响安全性。鉴于这项研究和其他研究的结果,应该重新考虑心导管插入术前的常规禁食。
A Randomized Trial of Cardiac Catheterization With Fasting Versus Liberal Oral Intake: The CALORI Trial
Background
Routine preprocedural fasting before cardiac catheterization remains common practice, despite a lack of robust evidence to support this practice. We investigated the impact of a liberal nonfasting strategy vs a standardized nil per os (NPO) regimen prior to cardiac catheterization.
Methods
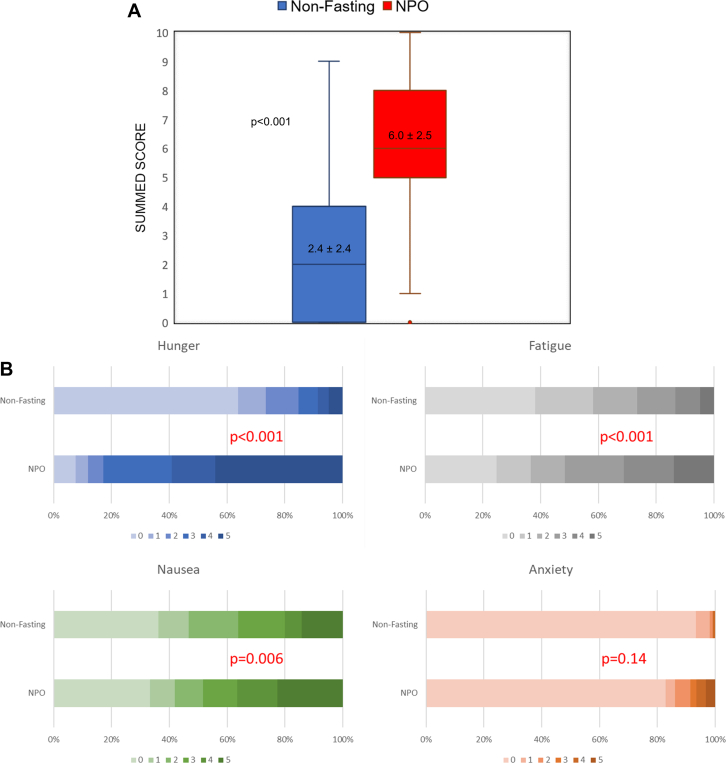
Adult inpatients undergoing elective or urgent cardiac catheterization were randomized (1:1 ratio) to either NPO past midnight or ad libitum intake of liquids and solids (without dietary constraints) until immediately prior to the procedure. Only patients at high risk of aspiration or undergoing complex interventions were excluded. The primary end point was preprocedural patient-reported well-being scores (scaled 0-5, with 0 signifying absence of ailment and 5 the most extreme form), for variables including hunger, fatigue, anxiety, and nausea. A composite score summed the individual scores for hunger and fatigue. Other end points were periprocedural adverse events including emesis, aspiration, or intubation, in addition to postprocedural satisfaction.
Results
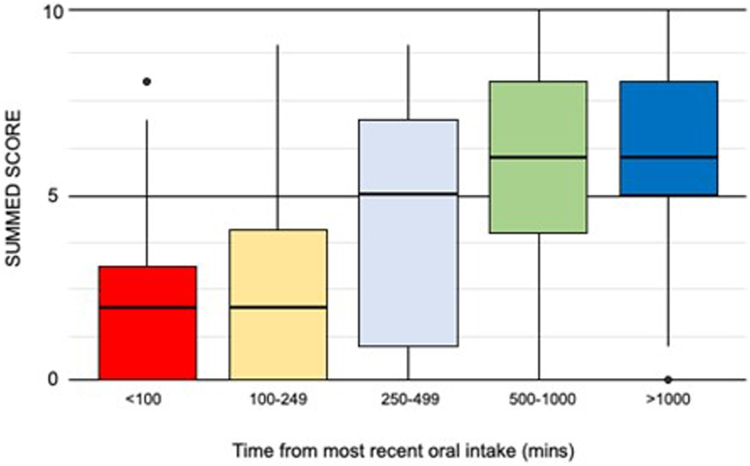
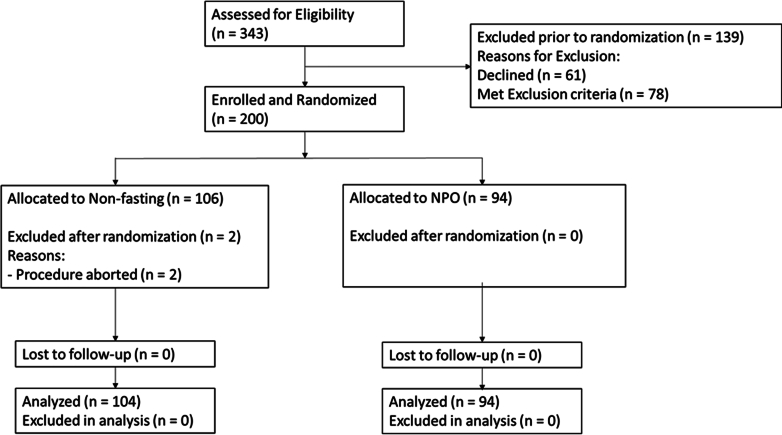
A total of 198 patients (65% male and 42% Black) were included in the final analysis. There were no differences in baseline characteristics between groups. Time from most recent oral intake (liquid or solid) to the start of the procedure averaged 148 minutes for the nonfasting group and 970 minutes for the NPO strategy (P < .001). The composite preprocedural well-being score was significantly better in the nonfasting arm (2.4 ± 2.4 nonfasting vs 6.0 ± 2.5 NPO; P < .001), as were the individual components of hunger (0.9 ± 1.5 vs 3.7 ± 1.5; P < .001), fatigue (1.5 ± 1.6 vs 2.3 ± 1.8; P < .001), and nausea (0.1 ± 0.5 vs 0.5 ±1.2; P = .006). There were no significant differences in adverse events between groups. Overall postprocedural satisfaction scores were significantly better in the nonfasting vs NPO group (0.3 ± 0.7 vs 1.0 ± 1.3, respectively; P < .001).
Conclusions
In this single-center randomized trial, a liberal nonfasting strategy prior to cardiac catheterization significantly improved patient well-being and satisfaction without compromising safety. Given the findings of this and other studies, routine fasting prior to cardiac catheterization should be reconsidered.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
