Wenyue Yang, Xiangran Feng, Jian Ni, Xin Zhang, Hui Yu, Xianghua Wu, Huijie Wang, Xinmin Zhao, Zhihuang Hu, Bo Yu, Yao Zhang, Ying Lin, Yi Xiang, Jialei Wang
{"title":"EGFR抑制剂联合达非尼和曲美替尼治疗EGFR突变肺癌患者及BRAFV600E突变介导的耐药:中国多中心真实世界经验","authors":"Wenyue Yang, Xiangran Feng, Jian Ni, Xin Zhang, Hui Yu, Xianghua Wu, Huijie Wang, Xinmin Zhao, Zhihuang Hu, Bo Yu, Yao Zhang, Ying Lin, Yi Xiang, Jialei Wang","doi":"10.21037/tlcr-24-803","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The combination therapy of the B-Raf proto-oncogene (BRAF) inhibitor dabrafenib and the mitogen-activated protein kinase kinase (MEK) inhibitor Trametinib has shown favorable outcomes in patients initially identified with BRAF<sup>V600E</sup> mutations. However, there are currently no large-scale study data focusing on the use of a triple therapy regimen of epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) plus dabrafenib and trametinib in patients with newly concomitant BRAF mutations after acquiring resistance to EGFR-TKIs. Our study aimed to explore the efficacy and safety of the triple therapy regimen through a multi-center real-world experience.</p><p><strong>Methods: </strong>We reviewed the medical records of 1,861 patients who were treated with EGFR-TKI targeted drugs at three major medical centers in Shanghai between June 2015 and August 2024. Among 1,288 patients who developed disease progression, we identified 14 patients who were treated with a triple therapy regimen of EGFR-TKI plus dabrafenib and trametinib due to newly acquired BRAF<sup>V600E</sup> mutation after EGFR-TKI resistance. The assessments comprised progression-free survival (PFS), overall survival (OS), objective response rate (ORR), disease control rate (DCR), and adverse events (AEs). We also performed further subgroup analysis to aid in identifying potential factors that influence treatment outcomes and enhance clinical decision-making.</p><p><strong>Results: </strong>At the time of the data cutoff (August 1, 2024), the estimated median PFS was 6.7 months [95% confidence interval (CI): 2.5-not evaluated (NE)]. The median OS was not reached in 14 patients. ORR was 35.7% (95% CI: 14.0-64.4%) and DCR was 78.6% (95% CI: 52.4-92.4%). Three patients (21.4%) reported progressive disease (PD) and that was the best response. The median PFS was 8.35 months (95% CI: 2.0-NE) in 8 patients receiving third-generation TKI followed by first-/second-generation EGFR-TKIs and 6.9 months (95% CI: 2.5-NE) in 6 patients receiving third-generation TKI as first-line treatment directly. There was no significant difference in PFS between the two groups of patients receiving third-generation TKIs in different treatment sequences above [hazard ratio (HR): 1.107; 95% CI: 0.318-3.854; P=0.85]. Subgroup analysis indicated that a complex genetic mutation background may be a potential factor contributing to poorer PFS. No unexpected adverse effects were reported. Apart from pyrexia, gastrointestinal-related adverse reactions and skin-related adverse reactions warrant close attention.</p><p><strong>Conclusions: </strong>The triple therapy regimen of EGFR-TKI plus dabrafenib and trametinib was found to have substantial and durable clinical benefit, with a manageable safety profile, in patients with newly concomitant BRAF<sup>V600E</sup> mutations after osimertinib failure.</p>","PeriodicalId":23271,"journal":{"name":"Translational lung cancer research","volume":"13 12","pages":"3500-3512"},"PeriodicalIF":3.5000,"publicationDate":"2024-12-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11736577/pdf/","citationCount":"0","resultStr":"{\"title\":\"EGFR inhibitors plus dabrafenib and trametinib in patients with EGFR-mutant lung cancer and resistance mediated by BRAF<sup>V600E</sup> mutation: a multi-center real-world experience in China.\",\"authors\":\"Wenyue Yang, Xiangran Feng, Jian Ni, Xin Zhang, Hui Yu, Xianghua Wu, Huijie Wang, Xinmin Zhao, Zhihuang Hu, Bo Yu, Yao Zhang, Ying Lin, Yi Xiang, Jialei Wang\",\"doi\":\"10.21037/tlcr-24-803\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The combination therapy of the B-Raf proto-oncogene (BRAF) inhibitor dabrafenib and the mitogen-activated protein kinase kinase (MEK) inhibitor Trametinib has shown favorable outcomes in patients initially identified with BRAF<sup>V600E</sup> mutations. However, there are currently no large-scale study data focusing on the use of a triple therapy regimen of epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) plus dabrafenib and trametinib in patients with newly concomitant BRAF mutations after acquiring resistance to EGFR-TKIs. Our study aimed to explore the efficacy and safety of the triple therapy regimen through a multi-center real-world experience.</p><p><strong>Methods: </strong>We reviewed the medical records of 1,861 patients who were treated with EGFR-TKI targeted drugs at three major medical centers in Shanghai between June 2015 and August 2024. Among 1,288 patients who developed disease progression, we identified 14 patients who were treated with a triple therapy regimen of EGFR-TKI plus dabrafenib and trametinib due to newly acquired BRAF<sup>V600E</sup> mutation after EGFR-TKI resistance. The assessments comprised progression-free survival (PFS), overall survival (OS), objective response rate (ORR), disease control rate (DCR), and adverse events (AEs). We also performed further subgroup analysis to aid in identifying potential factors that influence treatment outcomes and enhance clinical decision-making.</p><p><strong>Results: </strong>At the time of the data cutoff (August 1, 2024), the estimated median PFS was 6.7 months [95% confidence interval (CI): 2.5-not evaluated (NE)]. The median OS was not reached in 14 patients. ORR was 35.7% (95% CI: 14.0-64.4%) and DCR was 78.6% (95% CI: 52.4-92.4%). Three patients (21.4%) reported progressive disease (PD) and that was the best response. The median PFS was 8.35 months (95% CI: 2.0-NE) in 8 patients receiving third-generation TKI followed by first-/second-generation EGFR-TKIs and 6.9 months (95% CI: 2.5-NE) in 6 patients receiving third-generation TKI as first-line treatment directly. There was no significant difference in PFS between the two groups of patients receiving third-generation TKIs in different treatment sequences above [hazard ratio (HR): 1.107; 95% CI: 0.318-3.854; P=0.85]. Subgroup analysis indicated that a complex genetic mutation background may be a potential factor contributing to poorer PFS. No unexpected adverse effects were reported. Apart from pyrexia, gastrointestinal-related adverse reactions and skin-related adverse reactions warrant close attention.</p><p><strong>Conclusions: </strong>The triple therapy regimen of EGFR-TKI plus dabrafenib and trametinib was found to have substantial and durable clinical benefit, with a manageable safety profile, in patients with newly concomitant BRAF<sup>V600E</sup> mutations after osimertinib failure.</p>\",\"PeriodicalId\":23271,\"journal\":{\"name\":\"Translational lung cancer research\",\"volume\":\"13 12\",\"pages\":\"3500-3512\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2024-12-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11736577/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational lung cancer research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/tlcr-24-803\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/12/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational lung cancer research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tlcr-24-803","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
EGFR inhibitors plus dabrafenib and trametinib in patients with EGFR-mutant lung cancer and resistance mediated by BRAFV600E mutation: a multi-center real-world experience in China.
Background: The combination therapy of the B-Raf proto-oncogene (BRAF) inhibitor dabrafenib and the mitogen-activated protein kinase kinase (MEK) inhibitor Trametinib has shown favorable outcomes in patients initially identified with BRAFV600E mutations. However, there are currently no large-scale study data focusing on the use of a triple therapy regimen of epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) plus dabrafenib and trametinib in patients with newly concomitant BRAF mutations after acquiring resistance to EGFR-TKIs. Our study aimed to explore the efficacy and safety of the triple therapy regimen through a multi-center real-world experience.
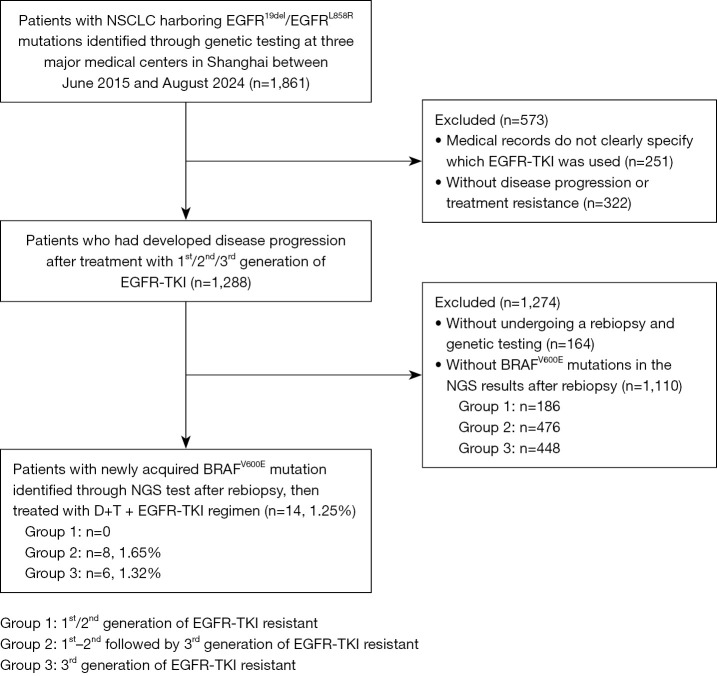
Methods: We reviewed the medical records of 1,861 patients who were treated with EGFR-TKI targeted drugs at three major medical centers in Shanghai between June 2015 and August 2024. Among 1,288 patients who developed disease progression, we identified 14 patients who were treated with a triple therapy regimen of EGFR-TKI plus dabrafenib and trametinib due to newly acquired BRAFV600E mutation after EGFR-TKI resistance. The assessments comprised progression-free survival (PFS), overall survival (OS), objective response rate (ORR), disease control rate (DCR), and adverse events (AEs). We also performed further subgroup analysis to aid in identifying potential factors that influence treatment outcomes and enhance clinical decision-making.
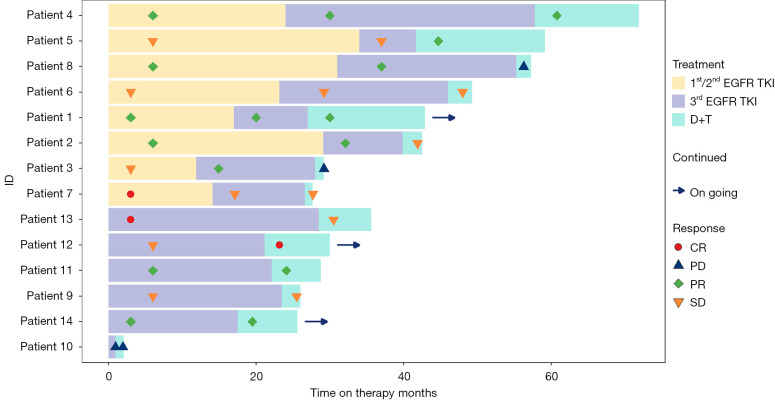
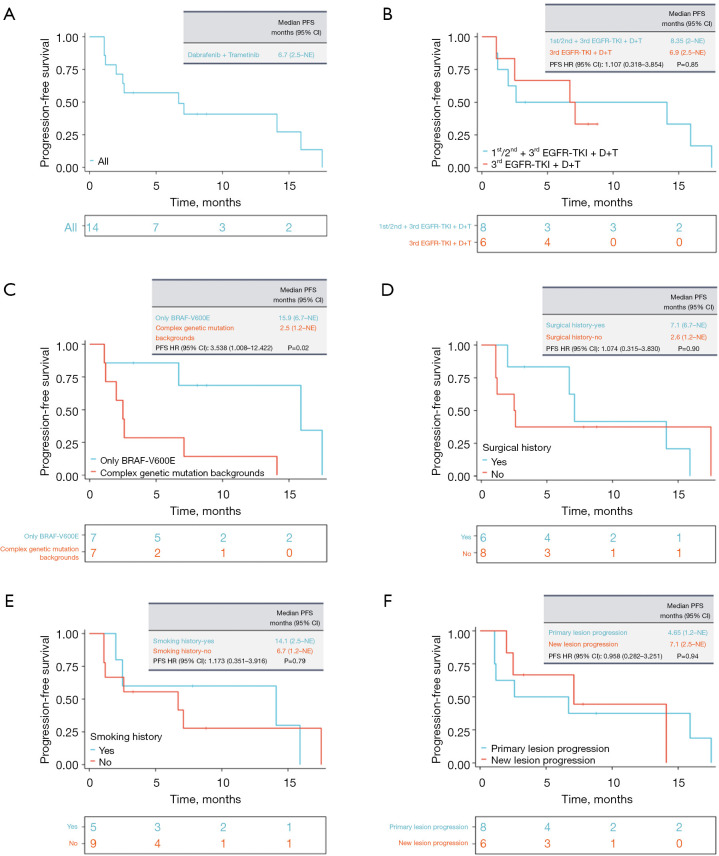
Results: At the time of the data cutoff (August 1, 2024), the estimated median PFS was 6.7 months [95% confidence interval (CI): 2.5-not evaluated (NE)]. The median OS was not reached in 14 patients. ORR was 35.7% (95% CI: 14.0-64.4%) and DCR was 78.6% (95% CI: 52.4-92.4%). Three patients (21.4%) reported progressive disease (PD) and that was the best response. The median PFS was 8.35 months (95% CI: 2.0-NE) in 8 patients receiving third-generation TKI followed by first-/second-generation EGFR-TKIs and 6.9 months (95% CI: 2.5-NE) in 6 patients receiving third-generation TKI as first-line treatment directly. There was no significant difference in PFS between the two groups of patients receiving third-generation TKIs in different treatment sequences above [hazard ratio (HR): 1.107; 95% CI: 0.318-3.854; P=0.85]. Subgroup analysis indicated that a complex genetic mutation background may be a potential factor contributing to poorer PFS. No unexpected adverse effects were reported. Apart from pyrexia, gastrointestinal-related adverse reactions and skin-related adverse reactions warrant close attention.
Conclusions: The triple therapy regimen of EGFR-TKI plus dabrafenib and trametinib was found to have substantial and durable clinical benefit, with a manageable safety profile, in patients with newly concomitant BRAFV600E mutations after osimertinib failure.
期刊介绍:
Translational Lung Cancer Research(TLCR, Transl Lung Cancer Res, Print ISSN 2218-6751; Online ISSN 2226-4477) is an international, peer-reviewed, open-access journal, which was founded in March 2012. TLCR is indexed by PubMed/PubMed Central and the Chemical Abstracts Service (CAS) Databases. It is published quarterly the first year, and published bimonthly since February 2013. It provides practical up-to-date information on prevention, early detection, diagnosis, and treatment of lung cancer. Specific areas of its interest include, but not limited to, multimodality therapy, markers, imaging, tumor biology, pathology, chemoprevention, and technical advances related to lung cancer.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
