Christopher J Wall, Richard N de Steiger, Christopher J Vertullo, Dylan Harries, Srinivas Kondalsamy-Chennakesavan
{"title":"ASA分级比BMI更能预测初次全膝关节置换术后早期翻修风险。","authors":"Christopher J Wall, Richard N de Steiger, Christopher J Vertullo, Dylan Harries, Srinivas Kondalsamy-Chennakesavan","doi":"10.2106/JBJS.OA.24.00064","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Although there is a known correlation between obesity and revision risk following total knee arthroplasty (TKA), there is an ongoing debate regarding the appropriateness of denying TKA solely based on the body mass index (BMI) of a patient. Our aim was to determine whether a patient's American Society of Anesthesiologists (ASA) class predicts their risks of early all-cause revision and revision for periprosthetic joint infection (PJI) following primary TKA, independent of their BMI.</p><p><strong>Methods: </strong>Data from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) were obtained regarding all patients who underwent primary TKA for osteoarthritis in Australia from January 1, 2015, to December 31, 2022. Estimated hazard ratios of all-cause revision and revision for PJI, as well as predicted risks of revision within 3 months, 1 year, and 2 years, as a function of patient ASA class and BMI, were calculated with use of multivariable Cox proportional hazards models.</p><p><strong>Results: </strong>A total of 274,786 primary TKAs (54.5% female; mean age, 68.3 years) were included in the study, of which 5,401 were revised during the study period. Compared with BMI, ASA class was a stronger predictor of the risks of all-cause revision and revision for PJI following primary TKA. Patients with an ASA class of 3 to 4 had higher risks of all-cause revision and revision for PJI at multiple time points after TKA compared with patients with an ASA class of 1 to 2, regardless of BMI.</p><p><strong>Conclusions: </strong>Although ASA class and BMI are theoretically interrelated variables, we found that a patient's ASA class was more strongly associated with their risks of early all-cause revision and revision for PJI following primary TKA than their BMI. Employing a BMI threshold in isolation when assessing fitness for TKA may be inappropriate, and surgeons should give greater weight to the other medical comorbidities and general perioperative fitness of the patient. Patients with poorly controlled comorbidities should be referred for medical optimization prior to TKA.</p><p><strong>Level of evidence: </strong>Prognostic Level III. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"10 1","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2025-01-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11737488/pdf/","citationCount":"0","resultStr":"{\"title\":\"ASA Class Is a Stronger Predictor of Early Revision Risk Following Primary Total Knee Arthroplasty than BMI.\",\"authors\":\"Christopher J Wall, Richard N de Steiger, Christopher J Vertullo, Dylan Harries, Srinivas Kondalsamy-Chennakesavan\",\"doi\":\"10.2106/JBJS.OA.24.00064\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Although there is a known correlation between obesity and revision risk following total knee arthroplasty (TKA), there is an ongoing debate regarding the appropriateness of denying TKA solely based on the body mass index (BMI) of a patient. Our aim was to determine whether a patient's American Society of Anesthesiologists (ASA) class predicts their risks of early all-cause revision and revision for periprosthetic joint infection (PJI) following primary TKA, independent of their BMI.</p><p><strong>Methods: </strong>Data from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) were obtained regarding all patients who underwent primary TKA for osteoarthritis in Australia from January 1, 2015, to December 31, 2022. Estimated hazard ratios of all-cause revision and revision for PJI, as well as predicted risks of revision within 3 months, 1 year, and 2 years, as a function of patient ASA class and BMI, were calculated with use of multivariable Cox proportional hazards models.</p><p><strong>Results: </strong>A total of 274,786 primary TKAs (54.5% female; mean age, 68.3 years) were included in the study, of which 5,401 were revised during the study period. Compared with BMI, ASA class was a stronger predictor of the risks of all-cause revision and revision for PJI following primary TKA. Patients with an ASA class of 3 to 4 had higher risks of all-cause revision and revision for PJI at multiple time points after TKA compared with patients with an ASA class of 1 to 2, regardless of BMI.</p><p><strong>Conclusions: </strong>Although ASA class and BMI are theoretically interrelated variables, we found that a patient's ASA class was more strongly associated with their risks of early all-cause revision and revision for PJI following primary TKA than their BMI. Employing a BMI threshold in isolation when assessing fitness for TKA may be inappropriate, and surgeons should give greater weight to the other medical comorbidities and general perioperative fitness of the patient. Patients with poorly controlled comorbidities should be referred for medical optimization prior to TKA.</p><p><strong>Level of evidence: </strong>Prognostic Level III. See Instructions for Authors for a complete description of levels of evidence.</p>\",\"PeriodicalId\":36492,\"journal\":{\"name\":\"JBJS Open Access\",\"volume\":\"10 1\",\"pages\":\"\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-01-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11737488/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JBJS Open Access\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2106/JBJS.OA.24.00064\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.24.00064","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
ASA Class Is a Stronger Predictor of Early Revision Risk Following Primary Total Knee Arthroplasty than BMI.
Background: Although there is a known correlation between obesity and revision risk following total knee arthroplasty (TKA), there is an ongoing debate regarding the appropriateness of denying TKA solely based on the body mass index (BMI) of a patient. Our aim was to determine whether a patient's American Society of Anesthesiologists (ASA) class predicts their risks of early all-cause revision and revision for periprosthetic joint infection (PJI) following primary TKA, independent of their BMI.
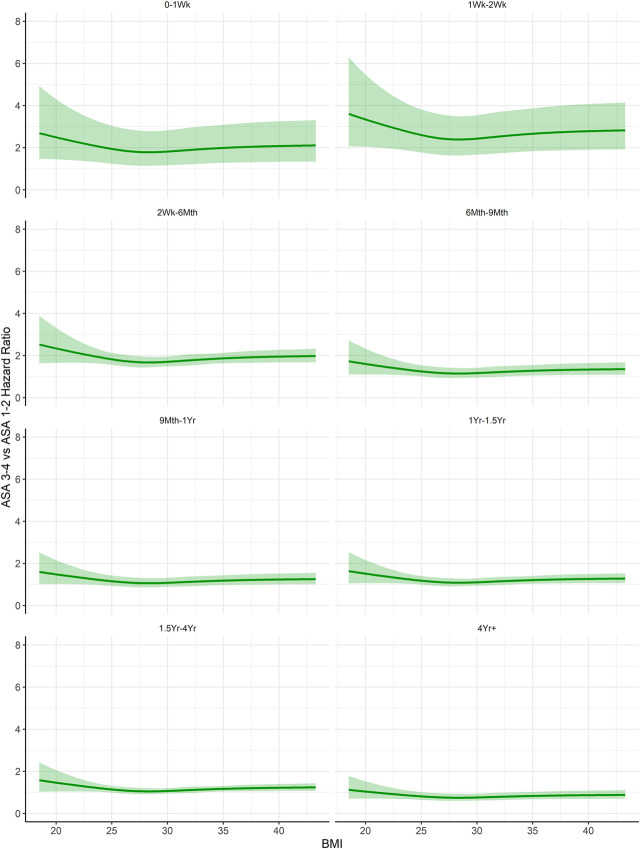
Methods: Data from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) were obtained regarding all patients who underwent primary TKA for osteoarthritis in Australia from January 1, 2015, to December 31, 2022. Estimated hazard ratios of all-cause revision and revision for PJI, as well as predicted risks of revision within 3 months, 1 year, and 2 years, as a function of patient ASA class and BMI, were calculated with use of multivariable Cox proportional hazards models.
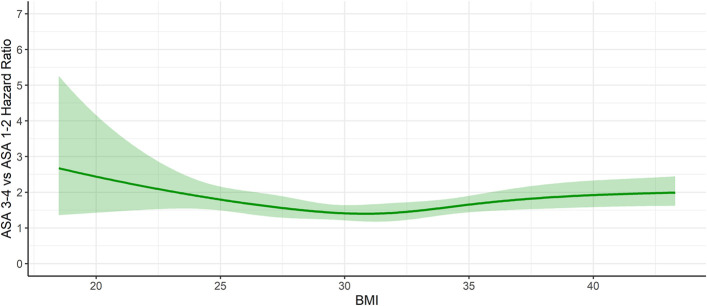
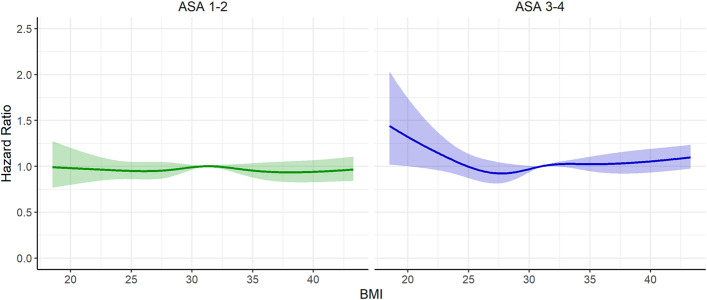
Results: A total of 274,786 primary TKAs (54.5% female; mean age, 68.3 years) were included in the study, of which 5,401 were revised during the study period. Compared with BMI, ASA class was a stronger predictor of the risks of all-cause revision and revision for PJI following primary TKA. Patients with an ASA class of 3 to 4 had higher risks of all-cause revision and revision for PJI at multiple time points after TKA compared with patients with an ASA class of 1 to 2, regardless of BMI.
Conclusions: Although ASA class and BMI are theoretically interrelated variables, we found that a patient's ASA class was more strongly associated with their risks of early all-cause revision and revision for PJI following primary TKA than their BMI. Employing a BMI threshold in isolation when assessing fitness for TKA may be inappropriate, and surgeons should give greater weight to the other medical comorbidities and general perioperative fitness of the patient. Patients with poorly controlled comorbidities should be referred for medical optimization prior to TKA.
Level of evidence: Prognostic Level III. See Instructions for Authors for a complete description of levels of evidence.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
