Christopher Tyson, Kevin H Li, Xiting Cao, James M O'Brien, Elliot K Fishman, Elizabeth K O'Donnell, Carlos Duran, Vijay Parthasarathy, Seema P Rego, Omair A Choudhry, Tomasz M Beer
{"title":"多癌早期检测试验的肿瘤定位策略:定量评估。","authors":"Christopher Tyson, Kevin H Li, Xiting Cao, James M O'Brien, Elliot K Fishman, Elizabeth K O'Donnell, Carlos Duran, Vijay Parthasarathy, Seema P Rego, Omair A Choudhry, Tomasz M Beer","doi":"10.1093/jncics/pkaf011","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Multicancer early detection tests may expand cancer screening. Characterizing diagnostic resolution approaches following positive multicancer early detection tests is critical. Two trials employed distinct resolution approaches: a molecular signal to predict tissue of origin and an imaging-based diagnostic strategy. This modeling study characterizes diagnostic journeys and impact in a hypothetical population of average-risk multicancer early detection-eligible patients.</p><p><strong>Methods: </strong>A mathematical expression for diagnostic burden was derived using positive predictive value (PPV), molecular tissue of origin localization accuracy, and numbers of procedures associated with each diagnostic outcome. Imaging-based and molecular tissue of origin-informed strategies were compared. Excess lifetime cancer risk due to futile radiation exposure was estimated using organ-specific diagnostic imaging radiation doses.</p><p><strong>Results: </strong>Across all PPVs and localization performances, a molecular tissue of origin strategy resulted in a higher diagnostic burden (mean = 3.6 [0.445] procedures vs mean = 2.6 [0.100] procedures) for the imaging strategy. Estimated diagnostic burden was higher for molecular tissue of origin in 95.5% of all PPV and tissue of origin accuracy combinations; at least 79% PPV and 90% accuracy would be required for a molecular tissue of origin-informed strategy to be less burdensome than imaging. The maximum rate of excess cancer incidence from radiation exposure for multicancer early detection false-positive results (individuals aged 50-84 years) was 64.6 of 100 000 (annual testing, 99% specificity), 48.5 of 100 000 (biennial testing, 98.5% specificity), and 64.6 of 100 000 (biennial testing, 98% specificity).</p><p><strong>Conclusions: </strong>An imaging-based diagnostic strategy is more efficient than a molecular tissue of origin-informed approach across almost all PPV and tissue of origin accuracy combinations. The use of an imaging-based approach for cancer localization can be efficient and low-risk compared with a molecular-informed approach.</p>","PeriodicalId":14681,"journal":{"name":"JNCI Cancer Spectrum","volume":" ","pages":""},"PeriodicalIF":4.1000,"publicationDate":"2025-03-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11897890/pdf/","citationCount":"0","resultStr":"{\"title\":\"Tumor localization strategies of multicancer early detection tests: a quantitative assessment.\",\"authors\":\"Christopher Tyson, Kevin H Li, Xiting Cao, James M O'Brien, Elliot K Fishman, Elizabeth K O'Donnell, Carlos Duran, Vijay Parthasarathy, Seema P Rego, Omair A Choudhry, Tomasz M Beer\",\"doi\":\"10.1093/jncics/pkaf011\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Multicancer early detection tests may expand cancer screening. Characterizing diagnostic resolution approaches following positive multicancer early detection tests is critical. Two trials employed distinct resolution approaches: a molecular signal to predict tissue of origin and an imaging-based diagnostic strategy. This modeling study characterizes diagnostic journeys and impact in a hypothetical population of average-risk multicancer early detection-eligible patients.</p><p><strong>Methods: </strong>A mathematical expression for diagnostic burden was derived using positive predictive value (PPV), molecular tissue of origin localization accuracy, and numbers of procedures associated with each diagnostic outcome. Imaging-based and molecular tissue of origin-informed strategies were compared. Excess lifetime cancer risk due to futile radiation exposure was estimated using organ-specific diagnostic imaging radiation doses.</p><p><strong>Results: </strong>Across all PPVs and localization performances, a molecular tissue of origin strategy resulted in a higher diagnostic burden (mean = 3.6 [0.445] procedures vs mean = 2.6 [0.100] procedures) for the imaging strategy. Estimated diagnostic burden was higher for molecular tissue of origin in 95.5% of all PPV and tissue of origin accuracy combinations; at least 79% PPV and 90% accuracy would be required for a molecular tissue of origin-informed strategy to be less burdensome than imaging. The maximum rate of excess cancer incidence from radiation exposure for multicancer early detection false-positive results (individuals aged 50-84 years) was 64.6 of 100 000 (annual testing, 99% specificity), 48.5 of 100 000 (biennial testing, 98.5% specificity), and 64.6 of 100 000 (biennial testing, 98% specificity).</p><p><strong>Conclusions: </strong>An imaging-based diagnostic strategy is more efficient than a molecular tissue of origin-informed approach across almost all PPV and tissue of origin accuracy combinations. The use of an imaging-based approach for cancer localization can be efficient and low-risk compared with a molecular-informed approach.</p>\",\"PeriodicalId\":14681,\"journal\":{\"name\":\"JNCI Cancer Spectrum\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":4.1000,\"publicationDate\":\"2025-03-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11897890/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JNCI Cancer Spectrum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/jncics/pkaf011\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JNCI Cancer Spectrum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jncics/pkaf011","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Tumor localization strategies of multicancer early detection tests: a quantitative assessment.
Background: Multicancer early detection tests may expand cancer screening. Characterizing diagnostic resolution approaches following positive multicancer early detection tests is critical. Two trials employed distinct resolution approaches: a molecular signal to predict tissue of origin and an imaging-based diagnostic strategy. This modeling study characterizes diagnostic journeys and impact in a hypothetical population of average-risk multicancer early detection-eligible patients.
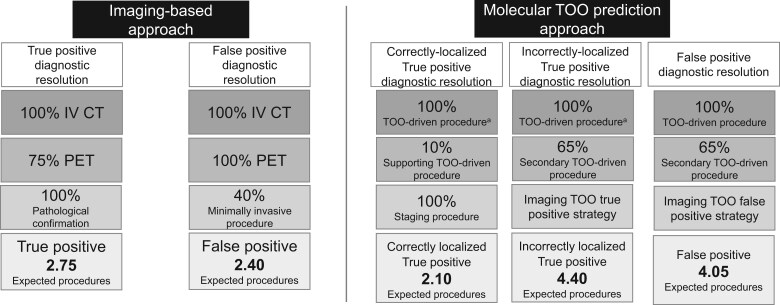
Methods: A mathematical expression for diagnostic burden was derived using positive predictive value (PPV), molecular tissue of origin localization accuracy, and numbers of procedures associated with each diagnostic outcome. Imaging-based and molecular tissue of origin-informed strategies were compared. Excess lifetime cancer risk due to futile radiation exposure was estimated using organ-specific diagnostic imaging radiation doses.
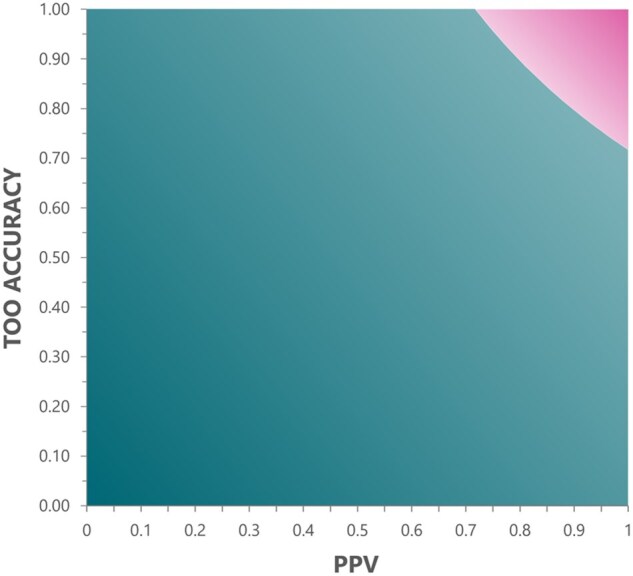
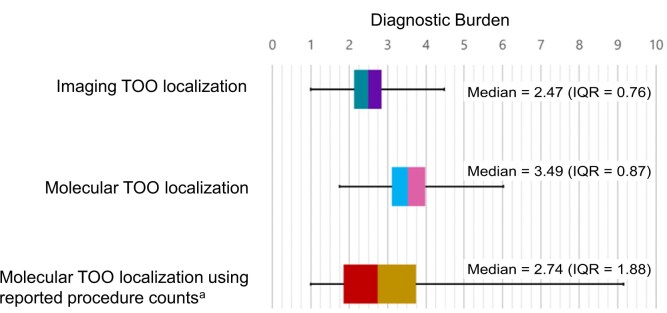
Results: Across all PPVs and localization performances, a molecular tissue of origin strategy resulted in a higher diagnostic burden (mean = 3.6 [0.445] procedures vs mean = 2.6 [0.100] procedures) for the imaging strategy. Estimated diagnostic burden was higher for molecular tissue of origin in 95.5% of all PPV and tissue of origin accuracy combinations; at least 79% PPV and 90% accuracy would be required for a molecular tissue of origin-informed strategy to be less burdensome than imaging. The maximum rate of excess cancer incidence from radiation exposure for multicancer early detection false-positive results (individuals aged 50-84 years) was 64.6 of 100 000 (annual testing, 99% specificity), 48.5 of 100 000 (biennial testing, 98.5% specificity), and 64.6 of 100 000 (biennial testing, 98% specificity).
Conclusions: An imaging-based diagnostic strategy is more efficient than a molecular tissue of origin-informed approach across almost all PPV and tissue of origin accuracy combinations. The use of an imaging-based approach for cancer localization can be efficient and low-risk compared with a molecular-informed approach.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
