Hyejo Ryu, Xue Li, Tae Hoon Lee, Tae Min Kim, Seung Hong Choi, Chul-Kee Park, Soon Tae Lee, Sung-Hye Park, Jae-Kyung Won, Bum-Sup Jang, Il Han Kim, Joo Ho Lee
{"title":"与海马有关的原发性中枢神经系统淋巴瘤的分布和失败模式:对海马避开照射的影响。","authors":"Hyejo Ryu, Xue Li, Tae Hoon Lee, Tae Min Kim, Seung Hong Choi, Chul-Kee Park, Soon Tae Lee, Sung-Hye Park, Jae-Kyung Won, Bum-Sup Jang, Il Han Kim, Joo Ho Lee","doi":"10.1007/s11060-025-04965-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Hippocampal injury from WBRT contributes to neurocognitive decline in brain malignancy patients. HA-WBRT may mitigate this by reducing hippocampal radiation exposure, but its feasibility in PCNSL remains unassessed regarding hippocampal involvement and failure rates. This study evaluates hippocampal involvement at diagnosis and after treatment in PCNSL patients.</p><p><strong>Materials and methods: </strong>We conducted a retrospective analysis of 278 immunocompetent PCNSL patients diagnosed between 2000 and 2021. Following high-dose methotrexate-based induction chemotherapy, patients either received consolidation therapy, including RT, cytarabine alone, or autologous stem cell transplantation or underwent observation. Hippocampus was outlined on T1 MRI images and expanded by a 5 mm margin to create the hippocampal avoidance region (HAR). Hippocampal failure was defined as recurrence or progression at HAR. The median follow-up was 38.7 months (range 3.1-239.4 months).</p><p><strong>Results: </strong>Of the 278 patients diagnosed with PCNSL, 39.9% presented initial lesions at HAR. After induction therapy, 212 evaluable patients received consolidation treatments or observation. Intracranial failures occurred in 47.6% (n = 101), with 66.3% (n = 67) occurring outside the HAR and 33.7% (n = 34) inside the HAR. Unifocal disease (HR 0.61, 95% CI 0.39-0.96, p = 0.025) was associated with a lower risk of hippocampal failures, while initial HAR involvement significantly increased the risk (HR 2.26, 95% CI 1.18-4.47, p = 0.018). Patients with unifocal disease outside the HAR had the lowest 3-year hippocampal failure rate (6.2%). RT that included the hippocampus did not significantly affect hippocampal failure rates in patients without initial HAR lesions (p = 0.282), with three-year rates of 9.2 vs. 14.6% for other treatments. However, among patients with initial HAR involvement, RT including the hippocampus significantly reduced hippocampal failure rates compared to other approaches (p = 0.002). Hippocampal failure rates were comparable, with conventional WBRT at 14.6% and HA-WBRT at 19% in patients without initial HAR lesions (p = 0.734).</p><p><strong>Conclusion: </strong>The routine application of the HA-WBRT strategy is not supported due to the high risk of hippocampal failures in general and requires further investigation to establish its feasibility and safety in well-defined subgroups. Our results suggest that the HA-WBRT strategy could be evaluated for select PCNSL patients with unifocal lesions or those located outside the HAR.</p>","PeriodicalId":16425,"journal":{"name":"Journal of Neuro-Oncology","volume":" ","pages":"95-104"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12041158/pdf/","citationCount":"0","resultStr":"{\"title\":\"Distribution and failure patterns of primary central nervous system lymphoma related to the hippocampus: implications for hippocampal avoidance irradiation.\",\"authors\":\"Hyejo Ryu, Xue Li, Tae Hoon Lee, Tae Min Kim, Seung Hong Choi, Chul-Kee Park, Soon Tae Lee, Sung-Hye Park, Jae-Kyung Won, Bum-Sup Jang, Il Han Kim, Joo Ho Lee\",\"doi\":\"10.1007/s11060-025-04965-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Hippocampal injury from WBRT contributes to neurocognitive decline in brain malignancy patients. HA-WBRT may mitigate this by reducing hippocampal radiation exposure, but its feasibility in PCNSL remains unassessed regarding hippocampal involvement and failure rates. This study evaluates hippocampal involvement at diagnosis and after treatment in PCNSL patients.</p><p><strong>Materials and methods: </strong>We conducted a retrospective analysis of 278 immunocompetent PCNSL patients diagnosed between 2000 and 2021. Following high-dose methotrexate-based induction chemotherapy, patients either received consolidation therapy, including RT, cytarabine alone, or autologous stem cell transplantation or underwent observation. Hippocampus was outlined on T1 MRI images and expanded by a 5 mm margin to create the hippocampal avoidance region (HAR). Hippocampal failure was defined as recurrence or progression at HAR. The median follow-up was 38.7 months (range 3.1-239.4 months).</p><p><strong>Results: </strong>Of the 278 patients diagnosed with PCNSL, 39.9% presented initial lesions at HAR. After induction therapy, 212 evaluable patients received consolidation treatments or observation. Intracranial failures occurred in 47.6% (n = 101), with 66.3% (n = 67) occurring outside the HAR and 33.7% (n = 34) inside the HAR. Unifocal disease (HR 0.61, 95% CI 0.39-0.96, p = 0.025) was associated with a lower risk of hippocampal failures, while initial HAR involvement significantly increased the risk (HR 2.26, 95% CI 1.18-4.47, p = 0.018). Patients with unifocal disease outside the HAR had the lowest 3-year hippocampal failure rate (6.2%). RT that included the hippocampus did not significantly affect hippocampal failure rates in patients without initial HAR lesions (p = 0.282), with three-year rates of 9.2 vs. 14.6% for other treatments. However, among patients with initial HAR involvement, RT including the hippocampus significantly reduced hippocampal failure rates compared to other approaches (p = 0.002). Hippocampal failure rates were comparable, with conventional WBRT at 14.6% and HA-WBRT at 19% in patients without initial HAR lesions (p = 0.734).</p><p><strong>Conclusion: </strong>The routine application of the HA-WBRT strategy is not supported due to the high risk of hippocampal failures in general and requires further investigation to establish its feasibility and safety in well-defined subgroups. Our results suggest that the HA-WBRT strategy could be evaluated for select PCNSL patients with unifocal lesions or those located outside the HAR.</p>\",\"PeriodicalId\":16425,\"journal\":{\"name\":\"Journal of Neuro-Oncology\",\"volume\":\" \",\"pages\":\"95-104\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12041158/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neuro-Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11060-025-04965-7\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/2/19 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neuro-Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11060-025-04965-7","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/19 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:WBRT所致海马损伤与脑恶性肿瘤患者神经认知能力下降有关。HA-WBRT可能通过减少海马辐射暴露来缓解这种情况,但其在PCNSL中的可行性仍未评估海马受损伤和失败率。本研究评估了PCNSL患者在诊断和治疗后的海马受累情况。材料和方法:我们对2000年至2021年间诊断的278例免疫正常的PCNSL患者进行了回顾性分析。在以大剂量甲氨蝶呤为基础的诱导化疗后,患者接受巩固治疗,包括放疗、单用阿糖胞苷、自体干细胞移植或观察。在T1 MRI图像上勾勒出海马,并扩大5毫米边缘,形成海马回避区(HAR)。海马功能衰竭被定义为复发或进展。中位随访时间为38.7个月(3.1-239.4个月)。结果:278例确诊为PCNSL的患者中,39.9%在HAR出现初始病变。诱导治疗后,212例可评估患者接受巩固治疗或观察。颅内失败发生率为47.6% (n = 101),其中66.3% (n = 67)发生在HAR外,33.7% (n = 34)发生在HAR内。单灶性疾病(HR 0.61, 95% CI 0.39-0.96, p = 0.025)与较低的海马功能衰竭风险相关,而初始HAR受累显著增加了风险(HR 2.26, 95% CI 1.18-4.47, p = 0.018)。HAR以外的单灶性疾病患者的3年海马失败率最低(6.2%)。在没有初始HAR病变的患者中,包括海马体的RT对海马体失败率没有显著影响(p = 0.282),三年的失败率为9.2,而其他治疗的失败率为14.6%。然而,在最初有HAR介入的患者中,与其他入路相比,包括海马在内的RT显著降低了海马失败率(p = 0.002)。在没有初始HAR病变的患者中,常规WBRT的失败率为14.6%,HA-WBRT的失败率为19% (p = 0.734)。结论:HA-WBRT策略不支持常规应用,因为一般情况下海马功能衰竭的风险较高,需要进一步研究以确定其在明确亚组中的可行性和安全性。我们的研究结果表明,HA-WBRT策略可以用于评估有单灶病变或位于HAR外的PCNSL患者。
Distribution and failure patterns of primary central nervous system lymphoma related to the hippocampus: implications for hippocampal avoidance irradiation.
Purpose: Hippocampal injury from WBRT contributes to neurocognitive decline in brain malignancy patients. HA-WBRT may mitigate this by reducing hippocampal radiation exposure, but its feasibility in PCNSL remains unassessed regarding hippocampal involvement and failure rates. This study evaluates hippocampal involvement at diagnosis and after treatment in PCNSL patients.
Materials and methods: We conducted a retrospective analysis of 278 immunocompetent PCNSL patients diagnosed between 2000 and 2021. Following high-dose methotrexate-based induction chemotherapy, patients either received consolidation therapy, including RT, cytarabine alone, or autologous stem cell transplantation or underwent observation. Hippocampus was outlined on T1 MRI images and expanded by a 5 mm margin to create the hippocampal avoidance region (HAR). Hippocampal failure was defined as recurrence or progression at HAR. The median follow-up was 38.7 months (range 3.1-239.4 months).
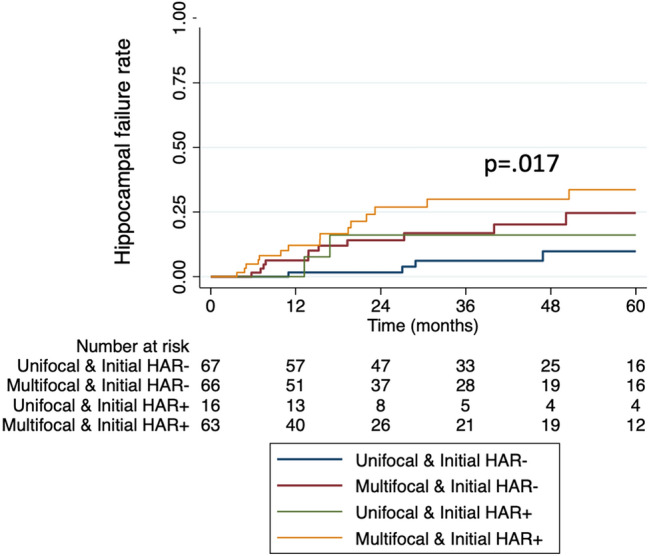
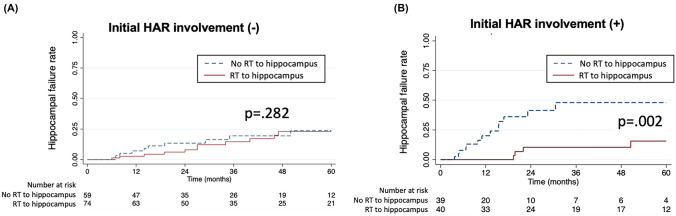
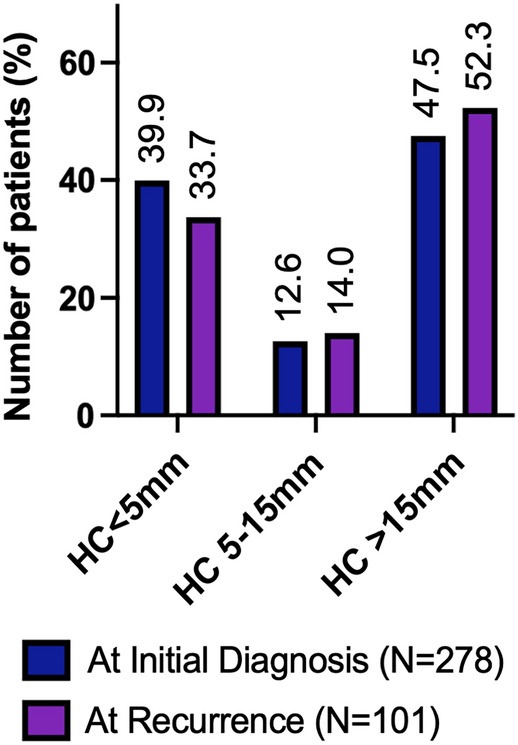
Results: Of the 278 patients diagnosed with PCNSL, 39.9% presented initial lesions at HAR. After induction therapy, 212 evaluable patients received consolidation treatments or observation. Intracranial failures occurred in 47.6% (n = 101), with 66.3% (n = 67) occurring outside the HAR and 33.7% (n = 34) inside the HAR. Unifocal disease (HR 0.61, 95% CI 0.39-0.96, p = 0.025) was associated with a lower risk of hippocampal failures, while initial HAR involvement significantly increased the risk (HR 2.26, 95% CI 1.18-4.47, p = 0.018). Patients with unifocal disease outside the HAR had the lowest 3-year hippocampal failure rate (6.2%). RT that included the hippocampus did not significantly affect hippocampal failure rates in patients without initial HAR lesions (p = 0.282), with three-year rates of 9.2 vs. 14.6% for other treatments. However, among patients with initial HAR involvement, RT including the hippocampus significantly reduced hippocampal failure rates compared to other approaches (p = 0.002). Hippocampal failure rates were comparable, with conventional WBRT at 14.6% and HA-WBRT at 19% in patients without initial HAR lesions (p = 0.734).
Conclusion: The routine application of the HA-WBRT strategy is not supported due to the high risk of hippocampal failures in general and requires further investigation to establish its feasibility and safety in well-defined subgroups. Our results suggest that the HA-WBRT strategy could be evaluated for select PCNSL patients with unifocal lesions or those located outside the HAR.
期刊介绍:
The Journal of Neuro-Oncology is a multi-disciplinary journal encompassing basic, applied, and clinical investigations in all research areas as they relate to cancer and the central nervous system. It provides a single forum for communication among neurologists, neurosurgeons, radiotherapists, medical oncologists, neuropathologists, neurodiagnosticians, and laboratory-based oncologists conducting relevant research. The Journal of Neuro-Oncology does not seek to isolate the field, but rather to focus the efforts of many disciplines in one publication through a format which pulls together these diverse interests. More than any other field of oncology, cancer of the central nervous system requires multi-disciplinary approaches. To alleviate having to scan dozens of journals of cell biology, pathology, laboratory and clinical endeavours, JNO is a periodical in which current, high-quality, relevant research in all aspects of neuro-oncology may be found.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
