Stefano Scotti, Lorenza Scotti, Federica Galimberti, Sining Xie, Manuela Casula, Elena Olmastroni
{"title":"多药治疗的操作性定义及其与全因住院风险的关系:使用行政数据库的概念框架。","authors":"Stefano Scotti, Lorenza Scotti, Federica Galimberti, Sining Xie, Manuela Casula, Elena Olmastroni","doi":"10.3390/pharmacy13010015","DOIUrl":null,"url":null,"abstract":"<p><p>Polypharmacy, defined as the concurrent use of multiple medications, increases the risk of various adverse outcomes. However, the variability in definitions across the literature contributes to substantial heterogeneity. Building on the published literature, this study aimed to identify a set of operational definitions of polypharmacy applicable to administrative databases and to assess their association with all-cause hospitalization. Data from the pharmacy refill and hospitalization databases of the Local Health Unit (LHU) of Bergamo, Lombardy, were analyzed. Patients aged ≥40 with at least one reimbursed drug prescription in 2017 were included. Prescription coverage was evaluated using total defined daily doses (DDDs), and all-cause hospitalizations from January to June 2018 were considered. Definitions explored included (i) the WHO's criterion of ≥5 medications by ATC fourth-level code; (ii) the exclusion of prescriptions usually for short-term treatments; and (iii) drugs with cumulative annual DDD ≥ 60. Approaches were assessed annually, quarterly, and monthly, and logistic regression was used to estimate odds ratios (ORs) for hospitalization risk. Among 431,620 patients, the DDD ≥ 60 definition showed the least variability (20.47-21.16%) and identified an older more complex cohort. All definitions showed a dose-dependent association with hospitalization risk. Different definitions of polypharmacy result in varying prevalence, with DDD ≥ 60 being the most consistent. A patient-centric approach is crucial to assess the appropriateness of polypharmacy.</p>","PeriodicalId":30544,"journal":{"name":"Pharmacy","volume":"13 1","pages":""},"PeriodicalIF":1.8000,"publicationDate":"2025-02-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11859879/pdf/","citationCount":"0","resultStr":"{\"title\":\"Operational Definitions of Polypharmacy and Their Association with All-Cause Hospitalization Risk: A Conceptual Framework Using Administrative Databases.\",\"authors\":\"Stefano Scotti, Lorenza Scotti, Federica Galimberti, Sining Xie, Manuela Casula, Elena Olmastroni\",\"doi\":\"10.3390/pharmacy13010015\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Polypharmacy, defined as the concurrent use of multiple medications, increases the risk of various adverse outcomes. However, the variability in definitions across the literature contributes to substantial heterogeneity. Building on the published literature, this study aimed to identify a set of operational definitions of polypharmacy applicable to administrative databases and to assess their association with all-cause hospitalization. Data from the pharmacy refill and hospitalization databases of the Local Health Unit (LHU) of Bergamo, Lombardy, were analyzed. Patients aged ≥40 with at least one reimbursed drug prescription in 2017 were included. Prescription coverage was evaluated using total defined daily doses (DDDs), and all-cause hospitalizations from January to June 2018 were considered. Definitions explored included (i) the WHO's criterion of ≥5 medications by ATC fourth-level code; (ii) the exclusion of prescriptions usually for short-term treatments; and (iii) drugs with cumulative annual DDD ≥ 60. Approaches were assessed annually, quarterly, and monthly, and logistic regression was used to estimate odds ratios (ORs) for hospitalization risk. Among 431,620 patients, the DDD ≥ 60 definition showed the least variability (20.47-21.16%) and identified an older more complex cohort. All definitions showed a dose-dependent association with hospitalization risk. Different definitions of polypharmacy result in varying prevalence, with DDD ≥ 60 being the most consistent. A patient-centric approach is crucial to assess the appropriateness of polypharmacy.</p>\",\"PeriodicalId\":30544,\"journal\":{\"name\":\"Pharmacy\",\"volume\":\"13 1\",\"pages\":\"\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-02-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11859879/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pharmacy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/pharmacy13010015\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/pharmacy13010015","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Operational Definitions of Polypharmacy and Their Association with All-Cause Hospitalization Risk: A Conceptual Framework Using Administrative Databases.
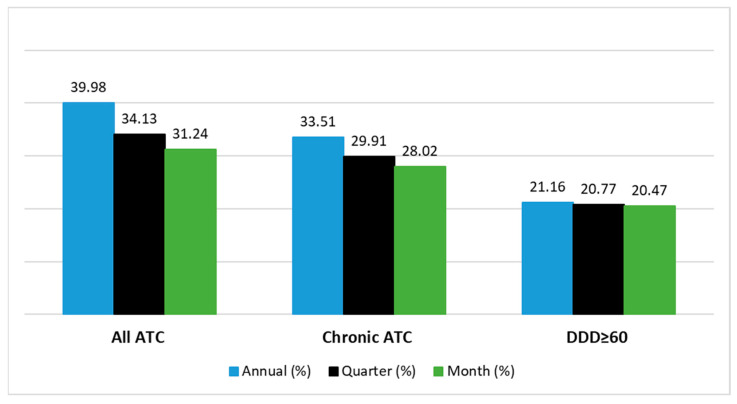
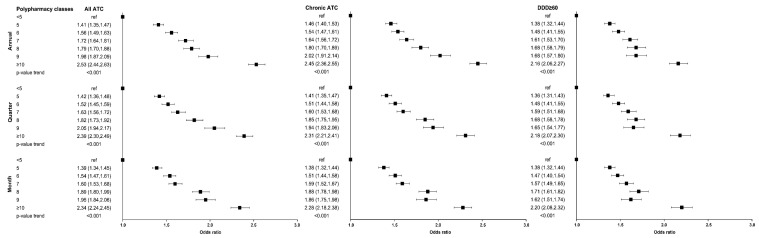
Polypharmacy, defined as the concurrent use of multiple medications, increases the risk of various adverse outcomes. However, the variability in definitions across the literature contributes to substantial heterogeneity. Building on the published literature, this study aimed to identify a set of operational definitions of polypharmacy applicable to administrative databases and to assess their association with all-cause hospitalization. Data from the pharmacy refill and hospitalization databases of the Local Health Unit (LHU) of Bergamo, Lombardy, were analyzed. Patients aged ≥40 with at least one reimbursed drug prescription in 2017 were included. Prescription coverage was evaluated using total defined daily doses (DDDs), and all-cause hospitalizations from January to June 2018 were considered. Definitions explored included (i) the WHO's criterion of ≥5 medications by ATC fourth-level code; (ii) the exclusion of prescriptions usually for short-term treatments; and (iii) drugs with cumulative annual DDD ≥ 60. Approaches were assessed annually, quarterly, and monthly, and logistic regression was used to estimate odds ratios (ORs) for hospitalization risk. Among 431,620 patients, the DDD ≥ 60 definition showed the least variability (20.47-21.16%) and identified an older more complex cohort. All definitions showed a dose-dependent association with hospitalization risk. Different definitions of polypharmacy result in varying prevalence, with DDD ≥ 60 being the most consistent. A patient-centric approach is crucial to assess the appropriateness of polypharmacy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
