Anna Zsofia Toth, Laszlo Nagy, Krisztina Maria Szabo, Vivien Racz, Alexandra Kiss, Gabor Sandorfi, Attila Borbely, Tibor Laszlo Nagy, Zoltan Csanadi
{"title":"早期心力衰竭住院或室性心律失常重新定义CRT后的远期预后。","authors":"Anna Zsofia Toth, Laszlo Nagy, Krisztina Maria Szabo, Vivien Racz, Alexandra Kiss, Gabor Sandorfi, Attila Borbely, Tibor Laszlo Nagy, Zoltan Csanadi","doi":"10.1002/ehf2.15274","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aims</h3>\n \n <p>Classifying patients as responders or non-responders to cardiac resynchronization therapy (CRT) has been recently challenged, suggesting that preventing heart failure (HF) progression may also provide survival benefits. We assessed a novel classification based on echocardiographic left ventricular (LV) reverse remodelling and the occurrence of acute HF hospitalization (HHF) or sustained ventricular arrhythmia (VA) within 1-year post-CRT.</p>\n </section>\n \n <section>\n \n <h3> Methods and results</h3>\n \n <p>Patients implanted with a CRT defibrillator (CRT-D) at our department between 2010 and 2020 were classified based on the change in LV ejection fraction (LVEF) within 1 year as responders (increase ≥ 10%), non-progressors (increase <10%) or progressors (decline). Patients in each category were further divided based on the occurrence or absence of an HHF/VA event within 1-year post-implantation. Long-term survival free of heart transplantation or LV assist device implantation was calculated for all six subgroups. Cohorts demonstrating no significant between-group differences were grouped together and reclassified as improved, stabilized or worsened. One hundred nineteen responders, 79 non-progressors and 69 progressors were identified based on the echocardiographic response. Long-term event-free survival was higher for responders as compared with non-progressors (hazard ratio [HR] 0.51, <i>P</i> = 0.002) or progressors (HR 0.34, <i>P</i> < 0.0001). Furthermore, non-progressors had better outcome than progressors (HR 0.63, <i>P</i> = 0.03). Long-term prognosis in patients was superior with versus without an HHF/VA event within each group of responders (HR 0.47, <i>P</i> = 0.03), non-progressors (HR 0.31, <i>P</i> = 0.0001) or progressors (HR 0.38, <i>P</i> = 0.0004). No survival difference was found between responders and non-progressors with no event (HR 0.69, <i>P</i> = 0.09), who were recategorized as improved. Long-term prognosis was also similar in responders with any event and in progressors with no event (HR 0.98, <i>P</i> = 0.88; stabilized), as well as in non-progressors and progressors with any event (HR 0.87, <i>P</i> = 0.63; worsened). Median survival rates demonstrated significant differences between the improved, stabilized and worsened groups (102.3, 62.0 and 24.4 months; HR 0.53, <i>P</i> = 0.006 between improved and stabilized; HR 0.41, <i>P</i> < 0.0001 between stabilized and worsened; HR 0.21, <i>P</i> < 0.0001 between improved and worsened cohorts, respectively).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Long-term survival can be predicted based on the change in LVEF and on the occurrence of an HHF/VA event within 1-year after CRT-D implantation. Stabilized patients have significantly better prognosis as compared with the worsened group. Patients with strikingly poor prognosis can be identified using this assessment method.</p>\n </section>\n </div>","PeriodicalId":11864,"journal":{"name":"ESC Heart Failure","volume":"12 4","pages":"2780-2790"},"PeriodicalIF":3.7000,"publicationDate":"2025-03-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ehf2.15274","citationCount":"0","resultStr":"{\"title\":\"Early occurrence of heart failure hospitalization or ventricular arrhythmia re-define the long-term prognosis after CRT\",\"authors\":\"Anna Zsofia Toth, Laszlo Nagy, Krisztina Maria Szabo, Vivien Racz, Alexandra Kiss, Gabor Sandorfi, Attila Borbely, Tibor Laszlo Nagy, Zoltan Csanadi\",\"doi\":\"10.1002/ehf2.15274\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>Classifying patients as responders or non-responders to cardiac resynchronization therapy (CRT) has been recently challenged, suggesting that preventing heart failure (HF) progression may also provide survival benefits. We assessed a novel classification based on echocardiographic left ventricular (LV) reverse remodelling and the occurrence of acute HF hospitalization (HHF) or sustained ventricular arrhythmia (VA) within 1-year post-CRT.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and results</h3>\\n \\n <p>Patients implanted with a CRT defibrillator (CRT-D) at our department between 2010 and 2020 were classified based on the change in LV ejection fraction (LVEF) within 1 year as responders (increase ≥ 10%), non-progressors (increase <10%) or progressors (decline). Patients in each category were further divided based on the occurrence or absence of an HHF/VA event within 1-year post-implantation. Long-term survival free of heart transplantation or LV assist device implantation was calculated for all six subgroups. Cohorts demonstrating no significant between-group differences were grouped together and reclassified as improved, stabilized or worsened. One hundred nineteen responders, 79 non-progressors and 69 progressors were identified based on the echocardiographic response. Long-term event-free survival was higher for responders as compared with non-progressors (hazard ratio [HR] 0.51, <i>P</i> = 0.002) or progressors (HR 0.34, <i>P</i> < 0.0001). Furthermore, non-progressors had better outcome than progressors (HR 0.63, <i>P</i> = 0.03). Long-term prognosis in patients was superior with versus without an HHF/VA event within each group of responders (HR 0.47, <i>P</i> = 0.03), non-progressors (HR 0.31, <i>P</i> = 0.0001) or progressors (HR 0.38, <i>P</i> = 0.0004). No survival difference was found between responders and non-progressors with no event (HR 0.69, <i>P</i> = 0.09), who were recategorized as improved. Long-term prognosis was also similar in responders with any event and in progressors with no event (HR 0.98, <i>P</i> = 0.88; stabilized), as well as in non-progressors and progressors with any event (HR 0.87, <i>P</i> = 0.63; worsened). Median survival rates demonstrated significant differences between the improved, stabilized and worsened groups (102.3, 62.0 and 24.4 months; HR 0.53, <i>P</i> = 0.006 between improved and stabilized; HR 0.41, <i>P</i> < 0.0001 between stabilized and worsened; HR 0.21, <i>P</i> < 0.0001 between improved and worsened cohorts, respectively).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Long-term survival can be predicted based on the change in LVEF and on the occurrence of an HHF/VA event within 1-year after CRT-D implantation. Stabilized patients have significantly better prognosis as compared with the worsened group. Patients with strikingly poor prognosis can be identified using this assessment method.</p>\\n </section>\\n </div>\",\"PeriodicalId\":11864,\"journal\":{\"name\":\"ESC Heart Failure\",\"volume\":\"12 4\",\"pages\":\"2780-2790\"},\"PeriodicalIF\":3.7000,\"publicationDate\":\"2025-03-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ehf2.15274\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ESC Heart Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ehf2.15274\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ESC Heart Failure","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ehf2.15274","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Early occurrence of heart failure hospitalization or ventricular arrhythmia re-define the long-term prognosis after CRT
Aims
Classifying patients as responders or non-responders to cardiac resynchronization therapy (CRT) has been recently challenged, suggesting that preventing heart failure (HF) progression may also provide survival benefits. We assessed a novel classification based on echocardiographic left ventricular (LV) reverse remodelling and the occurrence of acute HF hospitalization (HHF) or sustained ventricular arrhythmia (VA) within 1-year post-CRT.
Methods and results
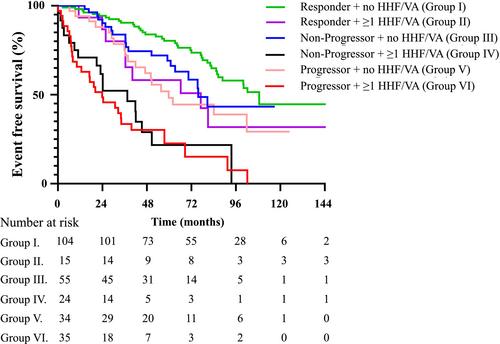
Patients implanted with a CRT defibrillator (CRT-D) at our department between 2010 and 2020 were classified based on the change in LV ejection fraction (LVEF) within 1 year as responders (increase ≥ 10%), non-progressors (increase <10%) or progressors (decline). Patients in each category were further divided based on the occurrence or absence of an HHF/VA event within 1-year post-implantation. Long-term survival free of heart transplantation or LV assist device implantation was calculated for all six subgroups. Cohorts demonstrating no significant between-group differences were grouped together and reclassified as improved, stabilized or worsened. One hundred nineteen responders, 79 non-progressors and 69 progressors were identified based on the echocardiographic response. Long-term event-free survival was higher for responders as compared with non-progressors (hazard ratio [HR] 0.51, P = 0.002) or progressors (HR 0.34, P < 0.0001). Furthermore, non-progressors had better outcome than progressors (HR 0.63, P = 0.03). Long-term prognosis in patients was superior with versus without an HHF/VA event within each group of responders (HR 0.47, P = 0.03), non-progressors (HR 0.31, P = 0.0001) or progressors (HR 0.38, P = 0.0004). No survival difference was found between responders and non-progressors with no event (HR 0.69, P = 0.09), who were recategorized as improved. Long-term prognosis was also similar in responders with any event and in progressors with no event (HR 0.98, P = 0.88; stabilized), as well as in non-progressors and progressors with any event (HR 0.87, P = 0.63; worsened). Median survival rates demonstrated significant differences between the improved, stabilized and worsened groups (102.3, 62.0 and 24.4 months; HR 0.53, P = 0.006 between improved and stabilized; HR 0.41, P < 0.0001 between stabilized and worsened; HR 0.21, P < 0.0001 between improved and worsened cohorts, respectively).
Conclusions
Long-term survival can be predicted based on the change in LVEF and on the occurrence of an HHF/VA event within 1-year after CRT-D implantation. Stabilized patients have significantly better prognosis as compared with the worsened group. Patients with strikingly poor prognosis can be identified using this assessment method.
期刊介绍:
ESC Heart Failure is the open access journal of the Heart Failure Association of the European Society of Cardiology dedicated to the advancement of knowledge in the field of heart failure. The journal aims to improve the understanding, prevention, investigation and treatment of heart failure. Molecular and cellular biology, pathology, physiology, electrophysiology, pharmacology, as well as the clinical, social and population sciences all form part of the discipline that is heart failure. Accordingly, submission of manuscripts on basic, translational, clinical and population sciences is invited. Original contributions on nursing, care of the elderly, primary care, health economics and other specialist fields related to heart failure are also welcome, as are case reports that highlight interesting aspects of heart failure care and treatment.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
