{"title":"初级保健中进行的药物评价对住院率和死亡率的影响:一项随机对照试验的观察性随访","authors":"Veronica Milos Nymberg, Cecilia Lenander, Beata Borgström Bolmsjö","doi":"10.2147/DHPS.S283708","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Drug-related problems among the elderly population are common and increasing. Multi-professional medication reviews (MR) have arisen as a method to optimize drug therapy for frail elderly patients. Research has not yet been able to show conclusive evidence of the effect of MRs on mortality or hospital admissions.</p><p><strong>Aim: </strong>The aim of this study was to assess the impact of MRs' on hospital admissions and mortality after six and 12 months in a frail population of 369 patients in primary care in a cohort from a randomized controlled study.</p><p><strong>Methods: </strong>Patients were blindly randomized to an intervention group (receiving MRs) and a control group (receiving usual care). Descriptive data on mortality and hospital admissions at six and 12 months were collected. Survival analysis was performed for time to death and time to the first hospital admission within 12 months.</p><p><strong>Results: </strong>An observational follow-up was performed in a cohort of 369 patients, previously randomized to an intervention group (182) and a control group (187). Most of the patients (75%) were females and lived in nursing homes. At six months, 50 patients of the baseline population (27%) in the control group had been admitted to hospital at least once, compared to 40 patients (21%) in the intervention group. At 12 months, the percentage had increased to 70 (37%) in the control group compared to 53 (29%) in the intervention group. Compared to usual care, we found that MRs reduced the risk of hospital admissions within 12 months by 42% (HR = 0.58, 95% CI 0.37-0.92, p=0.021), but found no difference in mortality (HR = 1.12, 95% CI 0.78-1.61, p=0.551) between the groups.</p><p><strong>Conclusion: </strong>We suggest that MRs should be recommended in the care of frail elderly patients with expected benefits on delayed hospital admissions. The study is registered at ClinicalTrials.gov, registration number NCT04040855, Unique Protocol ID 2018/8.</p>","PeriodicalId":11377,"journal":{"name":"Drug, Healthcare and Patient Safety","volume":"13 ","pages":"1-9"},"PeriodicalIF":3.4000,"publicationDate":"2021-01-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/83/65/dhps-13-1.PMC7850439.pdf","citationCount":"2","resultStr":"{\"title\":\"The Impact of Medication Reviews Conducted in Primary Care on Hospital Admissions and Mortality: An Observational Follow-Up of a Randomized Controlled Trial.\",\"authors\":\"Veronica Milos Nymberg, Cecilia Lenander, Beata Borgström Bolmsjö\",\"doi\":\"10.2147/DHPS.S283708\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Drug-related problems among the elderly population are common and increasing. Multi-professional medication reviews (MR) have arisen as a method to optimize drug therapy for frail elderly patients. Research has not yet been able to show conclusive evidence of the effect of MRs on mortality or hospital admissions.</p><p><strong>Aim: </strong>The aim of this study was to assess the impact of MRs' on hospital admissions and mortality after six and 12 months in a frail population of 369 patients in primary care in a cohort from a randomized controlled study.</p><p><strong>Methods: </strong>Patients were blindly randomized to an intervention group (receiving MRs) and a control group (receiving usual care). Descriptive data on mortality and hospital admissions at six and 12 months were collected. Survival analysis was performed for time to death and time to the first hospital admission within 12 months.</p><p><strong>Results: </strong>An observational follow-up was performed in a cohort of 369 patients, previously randomized to an intervention group (182) and a control group (187). Most of the patients (75%) were females and lived in nursing homes. At six months, 50 patients of the baseline population (27%) in the control group had been admitted to hospital at least once, compared to 40 patients (21%) in the intervention group. At 12 months, the percentage had increased to 70 (37%) in the control group compared to 53 (29%) in the intervention group. Compared to usual care, we found that MRs reduced the risk of hospital admissions within 12 months by 42% (HR = 0.58, 95% CI 0.37-0.92, p=0.021), but found no difference in mortality (HR = 1.12, 95% CI 0.78-1.61, p=0.551) between the groups.</p><p><strong>Conclusion: </strong>We suggest that MRs should be recommended in the care of frail elderly patients with expected benefits on delayed hospital admissions. The study is registered at ClinicalTrials.gov, registration number NCT04040855, Unique Protocol ID 2018/8.</p>\",\"PeriodicalId\":11377,\"journal\":{\"name\":\"Drug, Healthcare and Patient Safety\",\"volume\":\"13 \",\"pages\":\"1-9\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2021-01-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/83/65/dhps-13-1.PMC7850439.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drug, Healthcare and Patient Safety\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/DHPS.S283708\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug, Healthcare and Patient Safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/DHPS.S283708","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 2
摘要
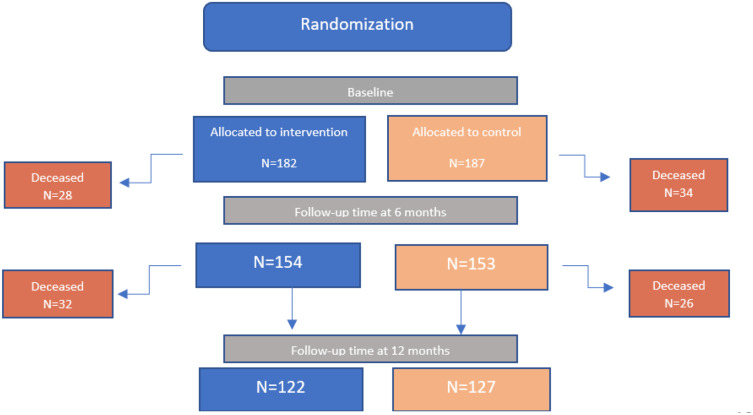
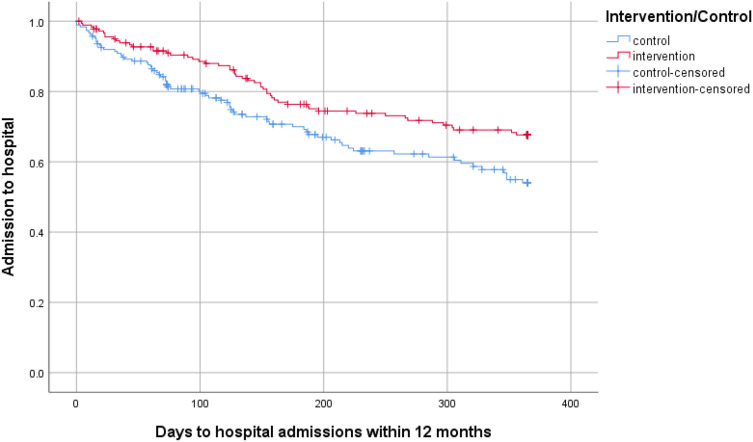
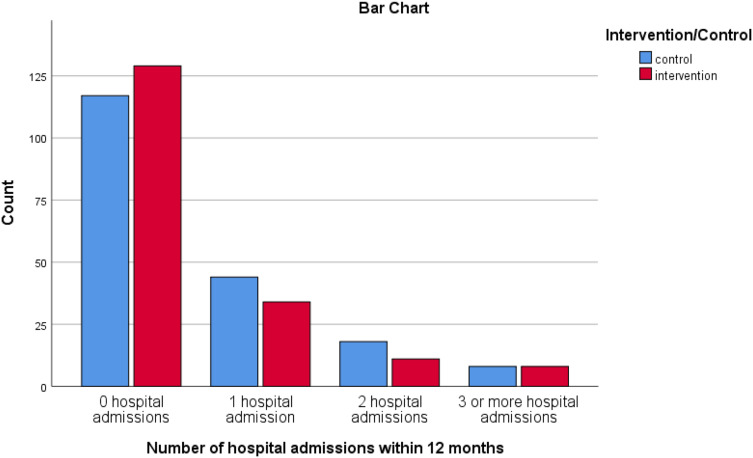
背景:与毒品有关的问题在老年人群中很常见,而且越来越多。多专业药物评价(MR)已成为优化老年体弱患者药物治疗的一种方法。研究还没有能够显示出mr对死亡率或住院率影响的确凿证据。目的:本研究的目的是在一项随机对照研究中,对369名接受初级保健的虚弱人群进行6个月和12个月后MRs对住院率和死亡率的影响。方法:将患者随机分为干预组(接受MRs治疗)和对照组(接受常规治疗)。收集了6个月和12个月时死亡率和住院率的描述性数据。对死亡时间和12个月内首次住院时间进行生存分析。结果:对369例患者进行了观察性随访,之前随机分为干预组(182例)和对照组(187例)。大多数患者(75%)是女性,住在养老院。6个月时,对照组基线人群中有50名患者(27%)至少住院一次,而干预组为40名患者(21%)。在12个月时,对照组的百分比增加到70(37%),而干预组为53(29%)。与常规护理相比,我们发现MRs使12个月内住院的风险降低了42% (HR = 0.58, 95% CI 0.37-0.92, p=0.021),但两组之间的死亡率没有差异(HR = 1.12, 95% CI 0.78-1.61, p=0.551)。结论:我们建议在延迟住院的体弱老年患者的护理中推荐MRs。该研究在ClinicalTrials.gov注册,注册号为NCT04040855,唯一协议ID为2018/8。
The Impact of Medication Reviews Conducted in Primary Care on Hospital Admissions and Mortality: An Observational Follow-Up of a Randomized Controlled Trial.
Background: Drug-related problems among the elderly population are common and increasing. Multi-professional medication reviews (MR) have arisen as a method to optimize drug therapy for frail elderly patients. Research has not yet been able to show conclusive evidence of the effect of MRs on mortality or hospital admissions.
Aim: The aim of this study was to assess the impact of MRs' on hospital admissions and mortality after six and 12 months in a frail population of 369 patients in primary care in a cohort from a randomized controlled study.
Methods: Patients were blindly randomized to an intervention group (receiving MRs) and a control group (receiving usual care). Descriptive data on mortality and hospital admissions at six and 12 months were collected. Survival analysis was performed for time to death and time to the first hospital admission within 12 months.
Results: An observational follow-up was performed in a cohort of 369 patients, previously randomized to an intervention group (182) and a control group (187). Most of the patients (75%) were females and lived in nursing homes. At six months, 50 patients of the baseline population (27%) in the control group had been admitted to hospital at least once, compared to 40 patients (21%) in the intervention group. At 12 months, the percentage had increased to 70 (37%) in the control group compared to 53 (29%) in the intervention group. Compared to usual care, we found that MRs reduced the risk of hospital admissions within 12 months by 42% (HR = 0.58, 95% CI 0.37-0.92, p=0.021), but found no difference in mortality (HR = 1.12, 95% CI 0.78-1.61, p=0.551) between the groups.
Conclusion: We suggest that MRs should be recommended in the care of frail elderly patients with expected benefits on delayed hospital admissions. The study is registered at ClinicalTrials.gov, registration number NCT04040855, Unique Protocol ID 2018/8.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
