Joana Eugénio Santos, Ana Gaspar, Sara Querido, Cristina Jorge, André Weigert, Henrique Mesquita Gabriel, António Martinho, Domingos Machado
{"title":"移植后早期肾静脉血栓的意外成功:1例报告及文献复习。","authors":"Joana Eugénio Santos, Ana Gaspar, Sara Querido, Cristina Jorge, André Weigert, Henrique Mesquita Gabriel, António Martinho, Domingos Machado","doi":"10.5414/CNCS110407","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Allograft renal vein thrombosis can cause graft loss during the early postoperative period. This diagnosis is sometimes elusive, requiring a strong suspicion. On the other hand, several authors have recognized risk factors for allograft renal vein thrombosis, but neither a preventive approach nor a treatment have been recommended for this complication.</p><p><strong>Case presentation: </strong>We present a case report of early allograft renal vein thrombosis, preceded by femoral common deep vein thrombosis in a recipient of a third kidney transplant. Despite femoral common deep vein thrombosis treatment with low-molecular-weight heparin and progressive improvement of renal function to a nadir serum creatinine of 0.51 mg/dL, the patient experienced a sudden episode of anuria on postoperative day 5. Doppler ultrasonography strongly suggested the diagnosis of allograft renal vein thrombosis. The patient underwent balloon catheter and aspiration venous thrombectomy, followed by unfractionated heparin perfusion. After 4 days of anuria and multiple blood transfusions, when allograft nephrectomy was contemplated, diuresis suddenly resumed. After 1 year of follow-up, the patient still has a normal renal function.</p><p><strong>Conclusion: </strong>This case report shows successful treatment of allograft renal vein thrombosis associated with deep vein thrombosis in the first week of transplantation, using balloon catheter and aspiration venous thrombectomy followed by perfusion of unfractionated heparin. The authors suggest this technique as a treatment option for transplant renal vein thrombosis. However, they reinforce the importance of individualized treatment and they remind that a delay may jeopardize the potential benefit of the procedure.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"9 ","pages":"19-25"},"PeriodicalIF":0.0000,"publicationDate":"2021-02-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7901358/pdf/","citationCount":"0","resultStr":"{\"title\":\"Unexpected success in early post-transplantation renal vein thrombosis: A case report and literature review.\",\"authors\":\"Joana Eugénio Santos, Ana Gaspar, Sara Querido, Cristina Jorge, André Weigert, Henrique Mesquita Gabriel, António Martinho, Domingos Machado\",\"doi\":\"10.5414/CNCS110407\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Allograft renal vein thrombosis can cause graft loss during the early postoperative period. This diagnosis is sometimes elusive, requiring a strong suspicion. On the other hand, several authors have recognized risk factors for allograft renal vein thrombosis, but neither a preventive approach nor a treatment have been recommended for this complication.</p><p><strong>Case presentation: </strong>We present a case report of early allograft renal vein thrombosis, preceded by femoral common deep vein thrombosis in a recipient of a third kidney transplant. Despite femoral common deep vein thrombosis treatment with low-molecular-weight heparin and progressive improvement of renal function to a nadir serum creatinine of 0.51 mg/dL, the patient experienced a sudden episode of anuria on postoperative day 5. Doppler ultrasonography strongly suggested the diagnosis of allograft renal vein thrombosis. The patient underwent balloon catheter and aspiration venous thrombectomy, followed by unfractionated heparin perfusion. After 4 days of anuria and multiple blood transfusions, when allograft nephrectomy was contemplated, diuresis suddenly resumed. After 1 year of follow-up, the patient still has a normal renal function.</p><p><strong>Conclusion: </strong>This case report shows successful treatment of allograft renal vein thrombosis associated with deep vein thrombosis in the first week of transplantation, using balloon catheter and aspiration venous thrombectomy followed by perfusion of unfractionated heparin. The authors suggest this technique as a treatment option for transplant renal vein thrombosis. However, they reinforce the importance of individualized treatment and they remind that a delay may jeopardize the potential benefit of the procedure.</p>\",\"PeriodicalId\":10398,\"journal\":{\"name\":\"Clinical Nephrology. Case Studies\",\"volume\":\"9 \",\"pages\":\"19-25\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-02-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7901358/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Nephrology. Case Studies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5414/CNCS110407\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110407","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Unexpected success in early post-transplantation renal vein thrombosis: A case report and literature review.
Background: Allograft renal vein thrombosis can cause graft loss during the early postoperative period. This diagnosis is sometimes elusive, requiring a strong suspicion. On the other hand, several authors have recognized risk factors for allograft renal vein thrombosis, but neither a preventive approach nor a treatment have been recommended for this complication.
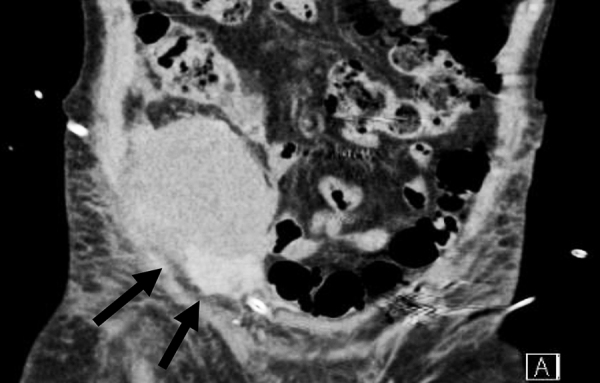
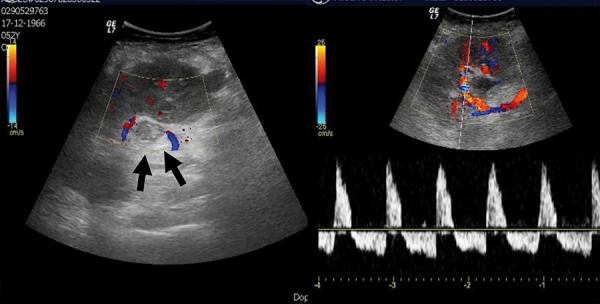
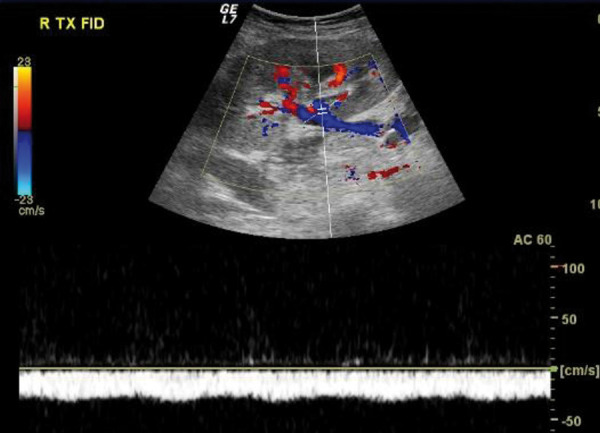
Case presentation: We present a case report of early allograft renal vein thrombosis, preceded by femoral common deep vein thrombosis in a recipient of a third kidney transplant. Despite femoral common deep vein thrombosis treatment with low-molecular-weight heparin and progressive improvement of renal function to a nadir serum creatinine of 0.51 mg/dL, the patient experienced a sudden episode of anuria on postoperative day 5. Doppler ultrasonography strongly suggested the diagnosis of allograft renal vein thrombosis. The patient underwent balloon catheter and aspiration venous thrombectomy, followed by unfractionated heparin perfusion. After 4 days of anuria and multiple blood transfusions, when allograft nephrectomy was contemplated, diuresis suddenly resumed. After 1 year of follow-up, the patient still has a normal renal function.
Conclusion: This case report shows successful treatment of allograft renal vein thrombosis associated with deep vein thrombosis in the first week of transplantation, using balloon catheter and aspiration venous thrombectomy followed by perfusion of unfractionated heparin. The authors suggest this technique as a treatment option for transplant renal vein thrombosis. However, they reinforce the importance of individualized treatment and they remind that a delay may jeopardize the potential benefit of the procedure.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
