Fredrik Ildstad, Hanne Ellekjær, Torgeir Wethal, Stian Lydersen, Hild Fjærtoft, Bent Indredavik
{"title":"TIA低卒中风险人群的ABCD3-I和ABCD2评分","authors":"Fredrik Ildstad, Hanne Ellekjær, Torgeir Wethal, Stian Lydersen, Hild Fjærtoft, Bent Indredavik","doi":"10.1155/2021/8845898","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>We aimed to evaluate the ABCD3-I score and compare it with the ABCD2 score in short- (1 week) and long-term (3 months; 1 year) stroke risk prediction in our post-TIA stroke risk study, MIDNOR TIA.</p><p><strong>Materials and methods: </strong>We performed a prospective, multicenter study in Central Norway from 2012 to 2015, enrolling 577 patients with TIA. In a subset of patients with complete data for both scores (<i>n</i> = 305), we calculated the AUC statistics of the ABCD3-I score and compared this with the ABCD2 score. A telephone follow-up and registry data were used for assessing stroke occurrence.</p><p><strong>Results: </strong>Within 1 week, 3 months, and 1 year, 1.0% (<i>n</i> = 3), 3.3% (<i>n</i> = 10), and 5.2% (<i>n</i> = 16) experienced a stroke, respectively. The AUCs for the ABCD3-I score were 0.72 (95% CI, 0.54 to 0.89) at 1 week, 0.66 (95% CI, 0.53 to 0.80) at 3 months, and 0.68 (0.95% CI, 0.56 to 0.79) at 1 year. The corresponding AUCs for the ABCD2 score were 0.55 (95% CI, 0.24 to 0.86), 0.55 (95% CI, 0.42 to 0.68), and 0.63 (95% CI, 0.50 to 0.76).</p><p><strong>Conclusions: </strong>The ABCD3-I score had limited value in a short-term prediction of subsequent stroke after TIA and did not reliably discriminate between low- and high-risk patients in a long-term follow-up. The ABCD2 score did not predict subsequent stroke accurately at any time point. Since there is a generally lower stroke risk after TIA during the last years, the benefit of these clinical risk scores and their role in TIA management seems limited. <i>Clinical Trial Registration</i>. This trial is registered with NCT02038725 (retrospectively registered, January 16, 2014).</p>","PeriodicalId":22054,"journal":{"name":"Stroke Research and Treatment","volume":"2021 ","pages":"8845898"},"PeriodicalIF":1.8000,"publicationDate":"2021-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7932764/pdf/","citationCount":"2","resultStr":"{\"title\":\"ABCD3-I and ABCD2 Scores in a TIA Population with Low Stroke Risk.\",\"authors\":\"Fredrik Ildstad, Hanne Ellekjær, Torgeir Wethal, Stian Lydersen, Hild Fjærtoft, Bent Indredavik\",\"doi\":\"10.1155/2021/8845898\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>We aimed to evaluate the ABCD3-I score and compare it with the ABCD2 score in short- (1 week) and long-term (3 months; 1 year) stroke risk prediction in our post-TIA stroke risk study, MIDNOR TIA.</p><p><strong>Materials and methods: </strong>We performed a prospective, multicenter study in Central Norway from 2012 to 2015, enrolling 577 patients with TIA. In a subset of patients with complete data for both scores (<i>n</i> = 305), we calculated the AUC statistics of the ABCD3-I score and compared this with the ABCD2 score. A telephone follow-up and registry data were used for assessing stroke occurrence.</p><p><strong>Results: </strong>Within 1 week, 3 months, and 1 year, 1.0% (<i>n</i> = 3), 3.3% (<i>n</i> = 10), and 5.2% (<i>n</i> = 16) experienced a stroke, respectively. The AUCs for the ABCD3-I score were 0.72 (95% CI, 0.54 to 0.89) at 1 week, 0.66 (95% CI, 0.53 to 0.80) at 3 months, and 0.68 (0.95% CI, 0.56 to 0.79) at 1 year. The corresponding AUCs for the ABCD2 score were 0.55 (95% CI, 0.24 to 0.86), 0.55 (95% CI, 0.42 to 0.68), and 0.63 (95% CI, 0.50 to 0.76).</p><p><strong>Conclusions: </strong>The ABCD3-I score had limited value in a short-term prediction of subsequent stroke after TIA and did not reliably discriminate between low- and high-risk patients in a long-term follow-up. The ABCD2 score did not predict subsequent stroke accurately at any time point. Since there is a generally lower stroke risk after TIA during the last years, the benefit of these clinical risk scores and their role in TIA management seems limited. <i>Clinical Trial Registration</i>. This trial is registered with NCT02038725 (retrospectively registered, January 16, 2014).</p>\",\"PeriodicalId\":22054,\"journal\":{\"name\":\"Stroke Research and Treatment\",\"volume\":\"2021 \",\"pages\":\"8845898\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2021-02-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7932764/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Stroke Research and Treatment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2021/8845898\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/8845898","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
ABCD3-I and ABCD2 Scores in a TIA Population with Low Stroke Risk.
Objectives: We aimed to evaluate the ABCD3-I score and compare it with the ABCD2 score in short- (1 week) and long-term (3 months; 1 year) stroke risk prediction in our post-TIA stroke risk study, MIDNOR TIA.
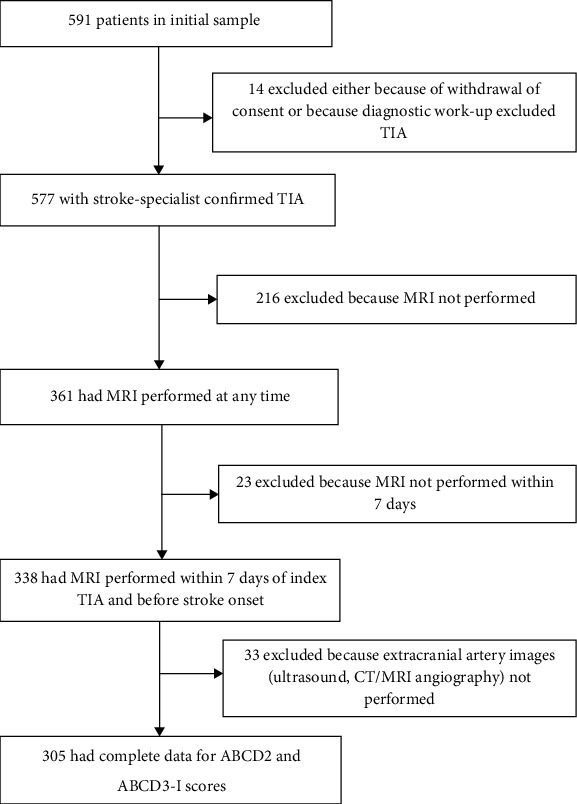
Materials and methods: We performed a prospective, multicenter study in Central Norway from 2012 to 2015, enrolling 577 patients with TIA. In a subset of patients with complete data for both scores (n = 305), we calculated the AUC statistics of the ABCD3-I score and compared this with the ABCD2 score. A telephone follow-up and registry data were used for assessing stroke occurrence.
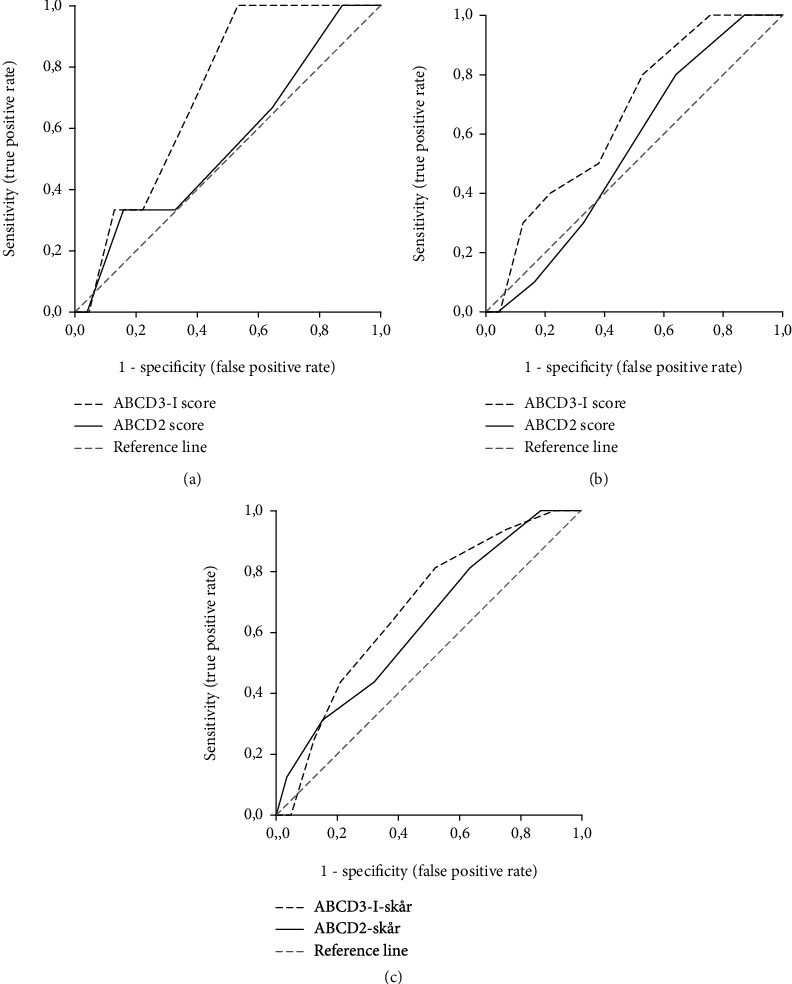
Results: Within 1 week, 3 months, and 1 year, 1.0% (n = 3), 3.3% (n = 10), and 5.2% (n = 16) experienced a stroke, respectively. The AUCs for the ABCD3-I score were 0.72 (95% CI, 0.54 to 0.89) at 1 week, 0.66 (95% CI, 0.53 to 0.80) at 3 months, and 0.68 (0.95% CI, 0.56 to 0.79) at 1 year. The corresponding AUCs for the ABCD2 score were 0.55 (95% CI, 0.24 to 0.86), 0.55 (95% CI, 0.42 to 0.68), and 0.63 (95% CI, 0.50 to 0.76).
Conclusions: The ABCD3-I score had limited value in a short-term prediction of subsequent stroke after TIA and did not reliably discriminate between low- and high-risk patients in a long-term follow-up. The ABCD2 score did not predict subsequent stroke accurately at any time point. Since there is a generally lower stroke risk after TIA during the last years, the benefit of these clinical risk scores and their role in TIA management seems limited. Clinical Trial Registration. This trial is registered with NCT02038725 (retrospectively registered, January 16, 2014).



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
