Dong-Kyu Moon, Ho-Seung Jo, Dong-Yeong Lee, Dong-Geun Kang, Hee-Chan Won, Min-Seok Seo, Sun-Chul Hwang
{"title":"前交叉韧带股骨隧道通过前内侧门静脉钻孔:三维平面钻孔角度影响隧道长度相对于切口成形术。","authors":"Dong-Kyu Moon, Ho-Seung Jo, Dong-Yeong Lee, Dong-Geun Kang, Hee-Chan Won, Min-Seok Seo, Sun-Chul Hwang","doi":"10.1186/s43019-021-00092-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Notchplasty is a surgical technique often performed during anterior cruciate ligament reconstruction (ACLR) with widening of the intercondylar notch of the lateral distal femur to avoid graft impingement. The purpose of this study was to correlate femoral-tunnel length with 3-dimensional (3D) drilling angle through the anteromedial (AM) portal with and without notchplasty.</p><p><strong>Materials and methods: </strong>Computer data were collected from an anatomical study using 16 cadaveric knees. The anterior cruciate ligament (ACL) femoral insertion was dissected and outlined for gross anatomical observation. The dissected cadaveric knees were scanned by computed tomography (CT). Three-dimensional measurements were calculated using software (Geomagic, Inc., Research Triangle Park, NC, USA) and included the center of the ACL footprint and the size of the ACL femoral footprint. The femoral-tunnel aperture centers were measured in the anatomical posterior-to-anterior and proximal-to-distal directions using Bernard's quadrant method. The ACL tunnel was created 3-demensionally in the anatomical center of femoral foot print of ACL using software (SolidWorks®, Corp., Waltham, MA, USA). The 8-mm cylinder shaped ACL tunnel was rested upon the anatomical center of the ACL footprint and placed in three different positions: the coronal plane, the sagittal plane, and the axial plane. Finally, the effect of notchplasty on the femoral-tunnel length and center of the ACL footprint were measured. All the above-mentioned studies performed ACLR using the AM portal.</p><p><strong>Results: </strong>The length of the femoral tunnels produced using the low coronal and high axial angles with 5-mm notchplasty became significantly shorter as the femoral starting position became more horizontal. The result was 30.38 ± 2.11 mm on average at 20° in the coronal plane/70° in the axial plane/45° in the sagittal plane and 31.26 ± 2.08 mm at 30° in the coronal plane/60° in the axial plane/45° in the sagittal plane, respectively, comparing the standard technique of 45° in the coronal/45° in the axial/45° in the sagittal plane of 32.98 ± 3.04 mm (P < 0.001). The tunnels made using the high coronal and low axial angles with notchplasty became longer than those made using the standard technique: 40.31 ± 3.36 mm at 60° in the coronal plane/30° in the axial plane/45° in the sagittal plane and 50.46 ± 3.13 mm at 75° in the coronal plane/15° in the axial plane/45° in the sagittal plane (P < 0.001).</p><p><strong>Conclusions: </strong>Our results show that excessive notchplasty causes the femoral tunnel to be located in the non-anatomical center of the ACL footprint and reduces the femoral-tunnel length. Therefore, care should be taken to avoid excessive notchplasty when performing this operation.</p>","PeriodicalId":17886,"journal":{"name":"Knee Surgery & Related Research","volume":"33 1","pages":"13"},"PeriodicalIF":4.9000,"publicationDate":"2021-04-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s43019-021-00092-5","citationCount":"6","resultStr":"{\"title\":\"Anterior cruciate ligament femoral-tunnel drilling through an anteromedial portal: 3-dimensional plane drilling angle affects tunnel length relative to notchplasty.\",\"authors\":\"Dong-Kyu Moon, Ho-Seung Jo, Dong-Yeong Lee, Dong-Geun Kang, Hee-Chan Won, Min-Seok Seo, Sun-Chul Hwang\",\"doi\":\"10.1186/s43019-021-00092-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Notchplasty is a surgical technique often performed during anterior cruciate ligament reconstruction (ACLR) with widening of the intercondylar notch of the lateral distal femur to avoid graft impingement. The purpose of this study was to correlate femoral-tunnel length with 3-dimensional (3D) drilling angle through the anteromedial (AM) portal with and without notchplasty.</p><p><strong>Materials and methods: </strong>Computer data were collected from an anatomical study using 16 cadaveric knees. The anterior cruciate ligament (ACL) femoral insertion was dissected and outlined for gross anatomical observation. The dissected cadaveric knees were scanned by computed tomography (CT). Three-dimensional measurements were calculated using software (Geomagic, Inc., Research Triangle Park, NC, USA) and included the center of the ACL footprint and the size of the ACL femoral footprint. The femoral-tunnel aperture centers were measured in the anatomical posterior-to-anterior and proximal-to-distal directions using Bernard's quadrant method. The ACL tunnel was created 3-demensionally in the anatomical center of femoral foot print of ACL using software (SolidWorks®, Corp., Waltham, MA, USA). The 8-mm cylinder shaped ACL tunnel was rested upon the anatomical center of the ACL footprint and placed in three different positions: the coronal plane, the sagittal plane, and the axial plane. Finally, the effect of notchplasty on the femoral-tunnel length and center of the ACL footprint were measured. All the above-mentioned studies performed ACLR using the AM portal.</p><p><strong>Results: </strong>The length of the femoral tunnels produced using the low coronal and high axial angles with 5-mm notchplasty became significantly shorter as the femoral starting position became more horizontal. The result was 30.38 ± 2.11 mm on average at 20° in the coronal plane/70° in the axial plane/45° in the sagittal plane and 31.26 ± 2.08 mm at 30° in the coronal plane/60° in the axial plane/45° in the sagittal plane, respectively, comparing the standard technique of 45° in the coronal/45° in the axial/45° in the sagittal plane of 32.98 ± 3.04 mm (P < 0.001). The tunnels made using the high coronal and low axial angles with notchplasty became longer than those made using the standard technique: 40.31 ± 3.36 mm at 60° in the coronal plane/30° in the axial plane/45° in the sagittal plane and 50.46 ± 3.13 mm at 75° in the coronal plane/15° in the axial plane/45° in the sagittal plane (P < 0.001).</p><p><strong>Conclusions: </strong>Our results show that excessive notchplasty causes the femoral tunnel to be located in the non-anatomical center of the ACL footprint and reduces the femoral-tunnel length. Therefore, care should be taken to avoid excessive notchplasty when performing this operation.</p>\",\"PeriodicalId\":17886,\"journal\":{\"name\":\"Knee Surgery & Related Research\",\"volume\":\"33 1\",\"pages\":\"13\"},\"PeriodicalIF\":4.9000,\"publicationDate\":\"2021-04-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s43019-021-00092-5\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Knee Surgery & Related Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s43019-021-00092-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Knee Surgery & Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43019-021-00092-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 6
摘要
背景:切迹成形术是前交叉韧带重建术(ACLR)中常用的一种外科技术,可扩大股骨外侧远端髁间切迹以避免移植物撞击。本研究的目的是在有无切口成形术的情况下,将股骨隧道长度与通过前内侧门静脉的三维(3D)钻孔角度联系起来。材料和方法:计算机数据来自16具尸体膝关节的解剖研究。解剖股骨前交叉韧带(ACL)止点并勾画大体解剖观察。对解剖的尸体膝关节进行计算机断层扫描(CT)。三维测量使用软件(Geomagic, Inc., Research Triangle Park, NC, USA)计算,包括前交叉韧带足迹的中心和前交叉韧带股骨足迹的大小。采用伯纳德象限法测量股骨-隧道孔中心的解剖后-前和近-远方向。使用软件(SolidWorks®,Corp., Waltham, MA, USA)在ACL股骨足印解剖中心三维创建ACL隧道。将8mm圆柱形ACL隧道放置在ACL足迹的解剖中心,并放置在冠状面、矢状面和轴向面三个不同的位置。最后,测量切口成形术对股骨隧道长度和前交叉韧带中心的影响。上述所有研究均使用AM门户进行ACLR。结果:低冠状角和高轴向角5-mm切口成形术的股骨隧道长度随着股骨起始位置的水平而明显缩短。结果冠状面20°/轴向70°/矢状面45°平均30.38±2.11 mm,冠状面30°/轴向60°/矢状面45°平均31.26±2.08 mm,与冠状面45°/轴向45°/矢状面45°的标准技术32.98±3.04 mm相比(P)。我们的研究结果表明,过度的切口成形术导致股骨隧道位于前交叉韧带的非解剖中心,并减少了股骨隧道的长度。因此,在进行该手术时应注意避免过度的切口成形。
Anterior cruciate ligament femoral-tunnel drilling through an anteromedial portal: 3-dimensional plane drilling angle affects tunnel length relative to notchplasty.
Background: Notchplasty is a surgical technique often performed during anterior cruciate ligament reconstruction (ACLR) with widening of the intercondylar notch of the lateral distal femur to avoid graft impingement. The purpose of this study was to correlate femoral-tunnel length with 3-dimensional (3D) drilling angle through the anteromedial (AM) portal with and without notchplasty.
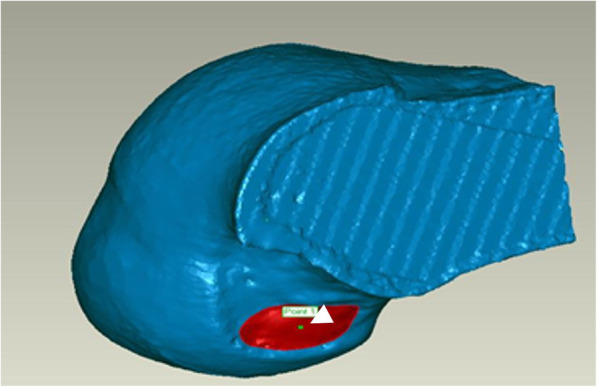
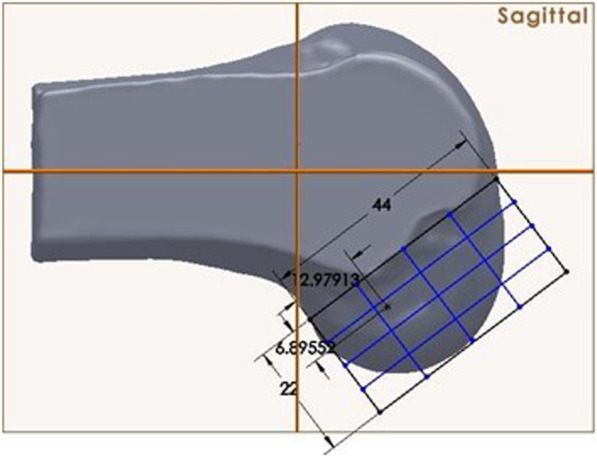
Materials and methods: Computer data were collected from an anatomical study using 16 cadaveric knees. The anterior cruciate ligament (ACL) femoral insertion was dissected and outlined for gross anatomical observation. The dissected cadaveric knees were scanned by computed tomography (CT). Three-dimensional measurements were calculated using software (Geomagic, Inc., Research Triangle Park, NC, USA) and included the center of the ACL footprint and the size of the ACL femoral footprint. The femoral-tunnel aperture centers were measured in the anatomical posterior-to-anterior and proximal-to-distal directions using Bernard's quadrant method. The ACL tunnel was created 3-demensionally in the anatomical center of femoral foot print of ACL using software (SolidWorks®, Corp., Waltham, MA, USA). The 8-mm cylinder shaped ACL tunnel was rested upon the anatomical center of the ACL footprint and placed in three different positions: the coronal plane, the sagittal plane, and the axial plane. Finally, the effect of notchplasty on the femoral-tunnel length and center of the ACL footprint were measured. All the above-mentioned studies performed ACLR using the AM portal.
Results: The length of the femoral tunnels produced using the low coronal and high axial angles with 5-mm notchplasty became significantly shorter as the femoral starting position became more horizontal. The result was 30.38 ± 2.11 mm on average at 20° in the coronal plane/70° in the axial plane/45° in the sagittal plane and 31.26 ± 2.08 mm at 30° in the coronal plane/60° in the axial plane/45° in the sagittal plane, respectively, comparing the standard technique of 45° in the coronal/45° in the axial/45° in the sagittal plane of 32.98 ± 3.04 mm (P < 0.001). The tunnels made using the high coronal and low axial angles with notchplasty became longer than those made using the standard technique: 40.31 ± 3.36 mm at 60° in the coronal plane/30° in the axial plane/45° in the sagittal plane and 50.46 ± 3.13 mm at 75° in the coronal plane/15° in the axial plane/45° in the sagittal plane (P < 0.001).
Conclusions: Our results show that excessive notchplasty causes the femoral tunnel to be located in the non-anatomical center of the ACL footprint and reduces the femoral-tunnel length. Therefore, care should be taken to avoid excessive notchplasty when performing this operation.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
