Luis Parodi MD, PhD, Eve Pickering PhD, Laura A. Cisar PhD, Doug Lee PhD, Raoudha Soufi-Mahjoubi MD
{"title":"预处理胆红素水平和UGT1A1多态性在伊立替康治疗前未治疗的结直肠癌患者中性粒细胞减少的多变量预测模型中的应用","authors":"Luis Parodi MD, PhD, Eve Pickering PhD, Laura A. Cisar PhD, Doug Lee PhD, Raoudha Soufi-Mahjoubi MD","doi":"10.1111/j.1753-5174.2008.00014.x","DOIUrl":null,"url":null,"abstract":"<p><b>Purpose. </b> Statistical models for predicting hematologic toxicity were evaluated based on <i>UGT1A1</i> polymorphisms and baseline serum bilirubin.</p><p><b>Methods. </b> Blood DNA samples were collected from 113 patients with untreated metastatic colorectal cancer receiving irinotecan (FOLFIRI, n = 36; mIFL, n = 41; CapeIRI, n = 36). The primary endpoint was absolute neutrophil count nadir during first treatment cycle. Linear regression models, with increased R<sup>2</sup> implying important additional predictive power, sequentially added age, sex, baseline bilirubin level, and <i>UGT1A1</i> genotype.</p><p><b>Results. </b> All models demonstrated low R<sup>2</sup>, suggesting unaccounted variables. <i>UGT1A1</i> genotype added ∼8–9% during cycle 1 and from ∼7% [mIFL regimen] to 26% [CapeIRI regimen] after cycle 1. Correlation between genotype and overall ANC nadir without regard to treatment was low (R = −0.201, <i>P</i> = 0.035). Patients with genotype 7/7 may have increased risk for severe neutropenia, but data are insufficient to characterize this. Contribution of baseline bilirubin level was negligible.</p><p><b>Conclusions. </b> Ability of <i>UGT1A1</i> or baseline bilirubin to predict neutropenia is low and depends on regimen.</p>","PeriodicalId":8181,"journal":{"name":"Archives of Drug Information","volume":"1 3","pages":"97-106"},"PeriodicalIF":0.0000,"publicationDate":"2008-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1111/j.1753-5174.2008.00014.x","citationCount":"6","resultStr":"{\"title\":\"Utility of Pretreatment Bilirubin Level and UGT1A1 Polymorphisms in Multivariate Predictive Models of Neutropenia Associated with Irinotecan Treatment in Previously Untreated Patients with Colorectal Cancer\",\"authors\":\"Luis Parodi MD, PhD, Eve Pickering PhD, Laura A. Cisar PhD, Doug Lee PhD, Raoudha Soufi-Mahjoubi MD\",\"doi\":\"10.1111/j.1753-5174.2008.00014.x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><b>Purpose. </b> Statistical models for predicting hematologic toxicity were evaluated based on <i>UGT1A1</i> polymorphisms and baseline serum bilirubin.</p><p><b>Methods. </b> Blood DNA samples were collected from 113 patients with untreated metastatic colorectal cancer receiving irinotecan (FOLFIRI, n = 36; mIFL, n = 41; CapeIRI, n = 36). The primary endpoint was absolute neutrophil count nadir during first treatment cycle. Linear regression models, with increased R<sup>2</sup> implying important additional predictive power, sequentially added age, sex, baseline bilirubin level, and <i>UGT1A1</i> genotype.</p><p><b>Results. </b> All models demonstrated low R<sup>2</sup>, suggesting unaccounted variables. <i>UGT1A1</i> genotype added ∼8–9% during cycle 1 and from ∼7% [mIFL regimen] to 26% [CapeIRI regimen] after cycle 1. Correlation between genotype and overall ANC nadir without regard to treatment was low (R = −0.201, <i>P</i> = 0.035). Patients with genotype 7/7 may have increased risk for severe neutropenia, but data are insufficient to characterize this. Contribution of baseline bilirubin level was negligible.</p><p><b>Conclusions. </b> Ability of <i>UGT1A1</i> or baseline bilirubin to predict neutropenia is low and depends on regimen.</p>\",\"PeriodicalId\":8181,\"journal\":{\"name\":\"Archives of Drug Information\",\"volume\":\"1 3\",\"pages\":\"97-106\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2008-12-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1111/j.1753-5174.2008.00014.x\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archives of Drug Information\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/j.1753-5174.2008.00014.x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Drug Information","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/j.1753-5174.2008.00014.x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 6
摘要
目的。基于UGT1A1多态性和基线血清胆红素,评估血液学毒性预测的统计模型。收集113例接受伊立替康治疗的未治疗的转移性结直肠癌患者的血液DNA样本(FOLFIRI, n = 36;mIFL, n = 41;CapeIRI, n = 36)。主要终点是第一个治疗周期中性粒细胞绝对计数最低点。线性回归模型,增加R2意味着重要的额外预测能力,依次增加年龄、性别、基线胆红素水平和UGT1A1基因型。所有模型均显示R2较低,表明存在未解释的变量。UGT1A1基因型在第1周期增加了~ 8-9%,在第1周期后从mIFL方案的~ 7%增加到CapeIRI方案的26%。基因型与总体ANC最低点不考虑治疗的相关性较低(R = - 0.201, P = 0.035)。基因型为7/7的患者发生严重中性粒细胞减少症的风险可能增加,但数据不足以说明这一点。基线胆红素水平的贡献可以忽略不计。UGT1A1或基线胆红素预测中性粒细胞减少的能力较低,且取决于治疗方案。
Utility of Pretreatment Bilirubin Level and UGT1A1 Polymorphisms in Multivariate Predictive Models of Neutropenia Associated with Irinotecan Treatment in Previously Untreated Patients with Colorectal Cancer
Purpose. Statistical models for predicting hematologic toxicity were evaluated based on UGT1A1 polymorphisms and baseline serum bilirubin.
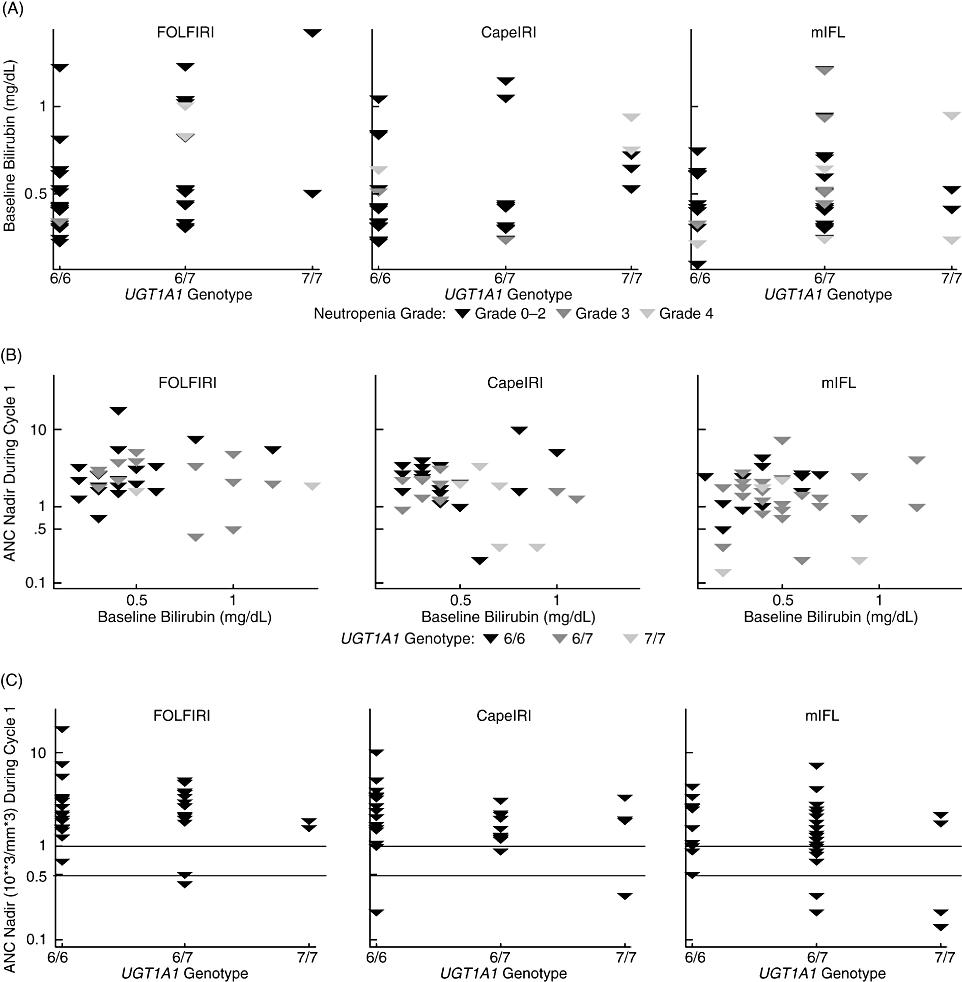
Methods. Blood DNA samples were collected from 113 patients with untreated metastatic colorectal cancer receiving irinotecan (FOLFIRI, n = 36; mIFL, n = 41; CapeIRI, n = 36). The primary endpoint was absolute neutrophil count nadir during first treatment cycle. Linear regression models, with increased R2 implying important additional predictive power, sequentially added age, sex, baseline bilirubin level, and UGT1A1 genotype.
Results. All models demonstrated low R2, suggesting unaccounted variables. UGT1A1 genotype added ∼8–9% during cycle 1 and from ∼7% [mIFL regimen] to 26% [CapeIRI regimen] after cycle 1. Correlation between genotype and overall ANC nadir without regard to treatment was low (R = −0.201, P = 0.035). Patients with genotype 7/7 may have increased risk for severe neutropenia, but data are insufficient to characterize this. Contribution of baseline bilirubin level was negligible.
Conclusions. Ability of UGT1A1 or baseline bilirubin to predict neutropenia is low and depends on regimen.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
