Mona Darwish PhD, Kenneth Tempero MD, PhD, John G. Jiang PhD, Philip G. Simonson PhD
{"title":"芬太尼含片不同给药方案在日本健康志愿者体内的相对生物利用度","authors":"Mona Darwish PhD, Kenneth Tempero MD, PhD, John G. Jiang PhD, Philip G. Simonson PhD","doi":"10.1111/j.1753-5174.2008.00009.x","DOIUrl":null,"url":null,"abstract":"<p><b>Background. </b> Fentanyl buccal tablet (FBT; <i>FENTORA</i><sup>®</sup>, Cephalon, Inc., Frazer, PA, USA) is indicated in the US for breakthrough pain in patients with cancer who are already receiving and are tolerant to around-the-clock opioid therapy for underlying persistent cancer pain. For each individual patient, FBT should be titrated to the effective dose.</p><p><b>Objective. </b> The primary objective was to characterize the pharmacokinetic parameters of FBT 400 µg administered as a single 400 µg tablet (regimen A) or as two 200 µg tablets given simultaneously (regimen B) and determine whether these are bioequivalent in healthy Japanese volunteers. Regimen C (two 200 µg tablets 30 minutes apart) was also compared as a secondary objective.</p><p><b>Methods. </b> Healthy Japanese adults received regimens A, B, and C in a crossover fashion. Naltrexone was given to minimize the opioid effects of fentanyl. Serum fentanyl concentrations were determined in venous blood collected through 36 hours post dose. Regimens were declared bioequivalent with respect to bioavailability (as reflected by AUC<sub>0–∞</sub>, AUC<sub>0–last</sub>, and C<sub>max</sub>) if the 90% confidence interval (CI) of the regimens' ratio fell within 0.80–1.25 (80%–125%).</p><p><b>Results. </b> Twenty-nine volunteers (13 men, 16 women) were enrolled; 24 completed the study. Regimens A and B had bioequivalent systemic exposure parameters (B/A [90% CI]: AUC<sub>0–∞</sub>108.4 [103.4, 113.7], AUC<sub>0–last</sub> 106.1 [100.7, 111.7], and C<sub>max</sub> 92.3 [83.2, 102.4]). Regimen C was bioequivalent to both A and B for AUCs, but only to B for C<sub>max</sub>. Median time to C<sub>max</sub> was 45 minutes for regimen A and 60 minutes for regimens B and C. The most frequent AEs were dizziness, application-site erythema, headache, somnolence, nausea, and vomiting. All AEs were mild or moderate.</p><p><b>Conclusions. </b> Bioavailability of fentanyl after FBT 400 µg administered as a single tablet was bioequivalent to that after 2 simultaneously administered 200 µg tablets in healthy Japanese volunteers. AEs were mild or moderate.</p>","PeriodicalId":8181,"journal":{"name":"Archives of Drug Information","volume":"1 2","pages":"56-62"},"PeriodicalIF":0.0000,"publicationDate":"2008-09-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1111/j.1753-5174.2008.00009.x","citationCount":"2","resultStr":"{\"title\":\"Relative Bioavailability of Fentanyl Following Various Dosing Regimens of Fentanyl Buccal Tablet in Healthy Japanese Volunteers\",\"authors\":\"Mona Darwish PhD, Kenneth Tempero MD, PhD, John G. Jiang PhD, Philip G. Simonson PhD\",\"doi\":\"10.1111/j.1753-5174.2008.00009.x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><b>Background. </b> Fentanyl buccal tablet (FBT; <i>FENTORA</i><sup>®</sup>, Cephalon, Inc., Frazer, PA, USA) is indicated in the US for breakthrough pain in patients with cancer who are already receiving and are tolerant to around-the-clock opioid therapy for underlying persistent cancer pain. For each individual patient, FBT should be titrated to the effective dose.</p><p><b>Objective. </b> The primary objective was to characterize the pharmacokinetic parameters of FBT 400 µg administered as a single 400 µg tablet (regimen A) or as two 200 µg tablets given simultaneously (regimen B) and determine whether these are bioequivalent in healthy Japanese volunteers. Regimen C (two 200 µg tablets 30 minutes apart) was also compared as a secondary objective.</p><p><b>Methods. </b> Healthy Japanese adults received regimens A, B, and C in a crossover fashion. Naltrexone was given to minimize the opioid effects of fentanyl. Serum fentanyl concentrations were determined in venous blood collected through 36 hours post dose. Regimens were declared bioequivalent with respect to bioavailability (as reflected by AUC<sub>0–∞</sub>, AUC<sub>0–last</sub>, and C<sub>max</sub>) if the 90% confidence interval (CI) of the regimens' ratio fell within 0.80–1.25 (80%–125%).</p><p><b>Results. </b> Twenty-nine volunteers (13 men, 16 women) were enrolled; 24 completed the study. Regimens A and B had bioequivalent systemic exposure parameters (B/A [90% CI]: AUC<sub>0–∞</sub>108.4 [103.4, 113.7], AUC<sub>0–last</sub> 106.1 [100.7, 111.7], and C<sub>max</sub> 92.3 [83.2, 102.4]). Regimen C was bioequivalent to both A and B for AUCs, but only to B for C<sub>max</sub>. Median time to C<sub>max</sub> was 45 minutes for regimen A and 60 minutes for regimens B and C. The most frequent AEs were dizziness, application-site erythema, headache, somnolence, nausea, and vomiting. All AEs were mild or moderate.</p><p><b>Conclusions. </b> Bioavailability of fentanyl after FBT 400 µg administered as a single tablet was bioequivalent to that after 2 simultaneously administered 200 µg tablets in healthy Japanese volunteers. AEs were mild or moderate.</p>\",\"PeriodicalId\":8181,\"journal\":{\"name\":\"Archives of Drug Information\",\"volume\":\"1 2\",\"pages\":\"56-62\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2008-09-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1111/j.1753-5174.2008.00009.x\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Archives of Drug Information\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/j.1753-5174.2008.00009.x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Archives of Drug Information","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/j.1753-5174.2008.00009.x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Relative Bioavailability of Fentanyl Following Various Dosing Regimens of Fentanyl Buccal Tablet in Healthy Japanese Volunteers
Background. Fentanyl buccal tablet (FBT; FENTORA®, Cephalon, Inc., Frazer, PA, USA) is indicated in the US for breakthrough pain in patients with cancer who are already receiving and are tolerant to around-the-clock opioid therapy for underlying persistent cancer pain. For each individual patient, FBT should be titrated to the effective dose.
Objective. The primary objective was to characterize the pharmacokinetic parameters of FBT 400 µg administered as a single 400 µg tablet (regimen A) or as two 200 µg tablets given simultaneously (regimen B) and determine whether these are bioequivalent in healthy Japanese volunteers. Regimen C (two 200 µg tablets 30 minutes apart) was also compared as a secondary objective.
Methods. Healthy Japanese adults received regimens A, B, and C in a crossover fashion. Naltrexone was given to minimize the opioid effects of fentanyl. Serum fentanyl concentrations were determined in venous blood collected through 36 hours post dose. Regimens were declared bioequivalent with respect to bioavailability (as reflected by AUC0–∞, AUC0–last, and Cmax) if the 90% confidence interval (CI) of the regimens' ratio fell within 0.80–1.25 (80%–125%).
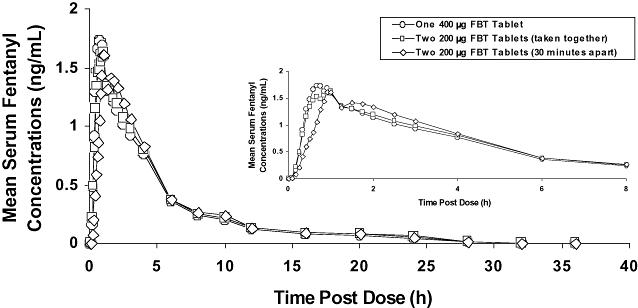
Results. Twenty-nine volunteers (13 men, 16 women) were enrolled; 24 completed the study. Regimens A and B had bioequivalent systemic exposure parameters (B/A [90% CI]: AUC0–∞108.4 [103.4, 113.7], AUC0–last 106.1 [100.7, 111.7], and Cmax 92.3 [83.2, 102.4]). Regimen C was bioequivalent to both A and B for AUCs, but only to B for Cmax. Median time to Cmax was 45 minutes for regimen A and 60 minutes for regimens B and C. The most frequent AEs were dizziness, application-site erythema, headache, somnolence, nausea, and vomiting. All AEs were mild or moderate.
Conclusions. Bioavailability of fentanyl after FBT 400 µg administered as a single tablet was bioequivalent to that after 2 simultaneously administered 200 µg tablets in healthy Japanese volunteers. AEs were mild or moderate.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
