{"title":"临床“记分卡”在管理咽喉痛患者中的作用。","authors":"Tony Mo Bakare, Peter Schattner","doi":"10.1186/1447-056X-9-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong></p><p><strong>Objective: </strong>To evaluate the usefulness of a clinical scorecard in managing sore throat in general practice.</p><p><strong>Design: </strong>Validation study of scorecard for sore throat with a throat swab culture used as the 'gold standard'.</p><p><strong>Setting: </strong>A solo family practice in rural New South Wales, AustraliaParticipants: Patients attending with sore throat.</p><p><strong>Methods: </strong>Patients from the age of 5 years and above presenting with the main symptom of a sore throat, and who have not had any antibiotic treatment in the previous two weeks, were invited to participate in the study. The doctor completed a scorecard for each patient participating and took a throat swab for culture. Adult patients (> 16 yrs) were asked to complete a patient satisfaction questionnaire, while guardians accompanying children (5 yr to < 16 yrs old) were asked to complete a similar, guardian questionnaire.</p><p><strong>Main outcome measures: </strong>1. Ability of a new scorecard to differentiate between bacterial and non-bacterial sore throat.2. Patients' trust in the scorecard.</p><p><strong>Results: </strong>The scorecard has a sensitivity of 93.33%, a specificity of 63.16%, a positive predictive value of 50% and a negative predictive value of 96%. The sensitivity is better than other sore throat scorecards that have been published but with a slightly lower specificity.There was a high level of patient trust in the scorecard was (85.8% agreement). Patients also trusted their doctor's judgement based on the scorecard (90.6% agreement).</p><p><strong>Conclusions: </strong>As the scorecard has a high sensitivity but only a moderate specificity, this means that it is more reliable for negative results, i.e. when the result suggests a viral infection. When the result favours a bacterial sore throat, then a high sensitivity can mean that there are a number of false positives. GPs can be confident in withholding antibiotics when the scorecard indicates a viral infection.</p>","PeriodicalId":39050,"journal":{"name":"Asia Pacific Family Medicine","volume":"9 1","pages":"9"},"PeriodicalIF":0.0000,"publicationDate":"2010-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1447-056X-9-9","citationCount":"4","resultStr":"{\"title\":\"The usefulness of a clinical 'scorecard' in managing patients with sore throat in general practice.\",\"authors\":\"Tony Mo Bakare, Peter Schattner\",\"doi\":\"10.1186/1447-056X-9-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong></p><p><strong>Objective: </strong>To evaluate the usefulness of a clinical scorecard in managing sore throat in general practice.</p><p><strong>Design: </strong>Validation study of scorecard for sore throat with a throat swab culture used as the 'gold standard'.</p><p><strong>Setting: </strong>A solo family practice in rural New South Wales, AustraliaParticipants: Patients attending with sore throat.</p><p><strong>Methods: </strong>Patients from the age of 5 years and above presenting with the main symptom of a sore throat, and who have not had any antibiotic treatment in the previous two weeks, were invited to participate in the study. The doctor completed a scorecard for each patient participating and took a throat swab for culture. Adult patients (> 16 yrs) were asked to complete a patient satisfaction questionnaire, while guardians accompanying children (5 yr to < 16 yrs old) were asked to complete a similar, guardian questionnaire.</p><p><strong>Main outcome measures: </strong>1. Ability of a new scorecard to differentiate between bacterial and non-bacterial sore throat.2. Patients' trust in the scorecard.</p><p><strong>Results: </strong>The scorecard has a sensitivity of 93.33%, a specificity of 63.16%, a positive predictive value of 50% and a negative predictive value of 96%. The sensitivity is better than other sore throat scorecards that have been published but with a slightly lower specificity.There was a high level of patient trust in the scorecard was (85.8% agreement). Patients also trusted their doctor's judgement based on the scorecard (90.6% agreement).</p><p><strong>Conclusions: </strong>As the scorecard has a high sensitivity but only a moderate specificity, this means that it is more reliable for negative results, i.e. when the result suggests a viral infection. When the result favours a bacterial sore throat, then a high sensitivity can mean that there are a number of false positives. GPs can be confident in withholding antibiotics when the scorecard indicates a viral infection.</p>\",\"PeriodicalId\":39050,\"journal\":{\"name\":\"Asia Pacific Family Medicine\",\"volume\":\"9 1\",\"pages\":\"9\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2010-07-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/1447-056X-9-9\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Asia Pacific Family Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/1447-056X-9-9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asia Pacific Family Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1447-056X-9-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
The usefulness of a clinical 'scorecard' in managing patients with sore throat in general practice.
Background:
Objective: To evaluate the usefulness of a clinical scorecard in managing sore throat in general practice.
Design: Validation study of scorecard for sore throat with a throat swab culture used as the 'gold standard'.
Setting: A solo family practice in rural New South Wales, AustraliaParticipants: Patients attending with sore throat.
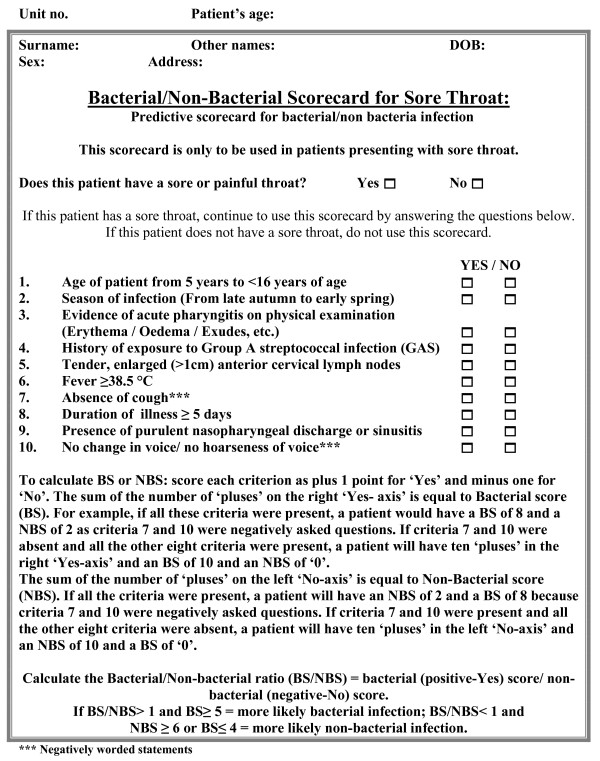
Methods: Patients from the age of 5 years and above presenting with the main symptom of a sore throat, and who have not had any antibiotic treatment in the previous two weeks, were invited to participate in the study. The doctor completed a scorecard for each patient participating and took a throat swab for culture. Adult patients (> 16 yrs) were asked to complete a patient satisfaction questionnaire, while guardians accompanying children (5 yr to < 16 yrs old) were asked to complete a similar, guardian questionnaire.
Main outcome measures: 1. Ability of a new scorecard to differentiate between bacterial and non-bacterial sore throat.2. Patients' trust in the scorecard.
Results: The scorecard has a sensitivity of 93.33%, a specificity of 63.16%, a positive predictive value of 50% and a negative predictive value of 96%. The sensitivity is better than other sore throat scorecards that have been published but with a slightly lower specificity.There was a high level of patient trust in the scorecard was (85.8% agreement). Patients also trusted their doctor's judgement based on the scorecard (90.6% agreement).
Conclusions: As the scorecard has a high sensitivity but only a moderate specificity, this means that it is more reliable for negative results, i.e. when the result suggests a viral infection. When the result favours a bacterial sore throat, then a high sensitivity can mean that there are a number of false positives. GPs can be confident in withholding antibiotics when the scorecard indicates a viral infection.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
