{"title":"恶性息肉结肠镜切除后切缘的价值及意义。","authors":"Eun Jung Jang, Dae Dong Kim, Chang Ho Cho","doi":"10.3393/jksc.2011.27.4.194","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study was designed to compare the clinicopathologic findings of an endoscopic polypectomy for malignant polyps with subsequent surgery and to evaluate the appropriateness of the pathologic finding criterion of the resection margin as an indicator for surgery in cases of malignant colorectal polyps.</p><p><strong>Methods: </strong>We examined the clinicopathologic characteristics, complications and prognoses among the patients who underwent a colonoscopic polypectomy in both our hospitals and at other hospitals from April 2003 and April 2010. These patients were divided into two groups, the group (non-operation group) that only underwent a polypectomy (n = 37) and the group (operation group) that underwent a polypectomy with subsequent surgery (n = 33).</p><p><strong>Results: </strong>There were no differences between two groups in the ratios of the number of men to the number of women, the ages or the comorbidities. In terms of endoscopic findings, we found no differences between the two groups in the locations of the polyps, the sizes of the polyps, or the presence of stalks. However, ulceration of polyps was higher in the non-operation group (51.5% vs. 21.6%; P = 0.009), as was the case with submucosal invasion (75.8% vs. 16.2%; P < 0.005). When an endoscopic polypectomy was performed, incomplete resection margins and specimens with margins involved occurred more frequently in the operation group (93.9% vs. 51.4%; P < 0.005), but no residual tumor was detected in 31 of 33 (93.9%) patients in that group. One pathologist reviewed the specimens of 54 patients (operation group, 19; non-operation group, 36). Six of the 19 polyps (31.6%) in the operation group and fifteen of the 36 polyps (41.7%) in the non-operation group had a margin without cancer cells.</p><p><strong>Conclusion: </strong>We may accept the criterion of a safe margin, including a coagulation zone. A multidisciplinary approach has to be developed by surgeons, endoscopists and pathologists based on a discussion of the risk factors for the patient before making a decision on the treatment treatment.</p>","PeriodicalId":17346,"journal":{"name":"Journal of the Korean Society of Coloproctology","volume":"27 4","pages":"194-201"},"PeriodicalIF":0.0000,"publicationDate":"2011-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/76/jksc-27-194.PMC3180600.pdf","citationCount":"6","resultStr":"{\"title\":\"Value and interpretation of resection margin after a colonoscopic polypectomy for malignant polyps.\",\"authors\":\"Eun Jung Jang, Dae Dong Kim, Chang Ho Cho\",\"doi\":\"10.3393/jksc.2011.27.4.194\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>This study was designed to compare the clinicopathologic findings of an endoscopic polypectomy for malignant polyps with subsequent surgery and to evaluate the appropriateness of the pathologic finding criterion of the resection margin as an indicator for surgery in cases of malignant colorectal polyps.</p><p><strong>Methods: </strong>We examined the clinicopathologic characteristics, complications and prognoses among the patients who underwent a colonoscopic polypectomy in both our hospitals and at other hospitals from April 2003 and April 2010. These patients were divided into two groups, the group (non-operation group) that only underwent a polypectomy (n = 37) and the group (operation group) that underwent a polypectomy with subsequent surgery (n = 33).</p><p><strong>Results: </strong>There were no differences between two groups in the ratios of the number of men to the number of women, the ages or the comorbidities. In terms of endoscopic findings, we found no differences between the two groups in the locations of the polyps, the sizes of the polyps, or the presence of stalks. However, ulceration of polyps was higher in the non-operation group (51.5% vs. 21.6%; P = 0.009), as was the case with submucosal invasion (75.8% vs. 16.2%; P < 0.005). When an endoscopic polypectomy was performed, incomplete resection margins and specimens with margins involved occurred more frequently in the operation group (93.9% vs. 51.4%; P < 0.005), but no residual tumor was detected in 31 of 33 (93.9%) patients in that group. One pathologist reviewed the specimens of 54 patients (operation group, 19; non-operation group, 36). Six of the 19 polyps (31.6%) in the operation group and fifteen of the 36 polyps (41.7%) in the non-operation group had a margin without cancer cells.</p><p><strong>Conclusion: </strong>We may accept the criterion of a safe margin, including a coagulation zone. A multidisciplinary approach has to be developed by surgeons, endoscopists and pathologists based on a discussion of the risk factors for the patient before making a decision on the treatment treatment.</p>\",\"PeriodicalId\":17346,\"journal\":{\"name\":\"Journal of the Korean Society of Coloproctology\",\"volume\":\"27 4\",\"pages\":\"194-201\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/c0/76/jksc-27-194.PMC3180600.pdf\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Korean Society of Coloproctology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3393/jksc.2011.27.4.194\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2011/8/31 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Korean Society of Coloproctology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3393/jksc.2011.27.4.194","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2011/8/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 6
摘要
目的:本研究旨在比较内镜下恶性息肉切除术与后续手术的临床病理表现,并评估切除边缘病理发现标准作为结直肠恶性息肉手术指标的适用性。方法:回顾性分析2003年4月至2010年4月在本院及外院行结肠镜息肉切除术患者的临床病理特点、并发症及预后。这些患者被分为两组,一组(非手术组)仅行息肉切除术(n = 37),另一组(手术组)行息肉切除术并随后手术(n = 33)。结果:两组患者在男女比例、年龄、合并症等方面均无差异。就内窥镜检查结果而言,我们发现两组在息肉的位置,息肉的大小或茎的存在方面没有差异。然而,非手术组的息肉溃疡发生率更高(51.5% vs. 21.6%;P = 0.009),粘膜下浸润也是如此(75.8% vs. 16.2%;P < 0.005)。内镜下息肉切除术时,术组边缘切除不全和边缘受累标本发生率更高(93.9% vs. 51.4%;P < 0.005),但该组33例患者中有31例(93.9%)未检出残留肿瘤。病理学家1人复查54例患者标本(手术组19例;非手术组,36例。手术组19例息肉中6例(31.6%),非手术组36例息肉中15例(41.7%)边缘无癌细胞。结论:我们可以接受包括凝血区在内的安全边界标准。外科医生、内窥镜医生和病理学家必须在对患者的危险因素进行讨论的基础上,制定一种多学科的治疗方法,然后再决定治疗方案。
Value and interpretation of resection margin after a colonoscopic polypectomy for malignant polyps.
Purpose: This study was designed to compare the clinicopathologic findings of an endoscopic polypectomy for malignant polyps with subsequent surgery and to evaluate the appropriateness of the pathologic finding criterion of the resection margin as an indicator for surgery in cases of malignant colorectal polyps.
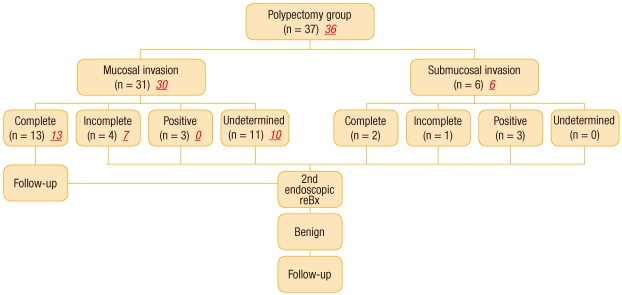
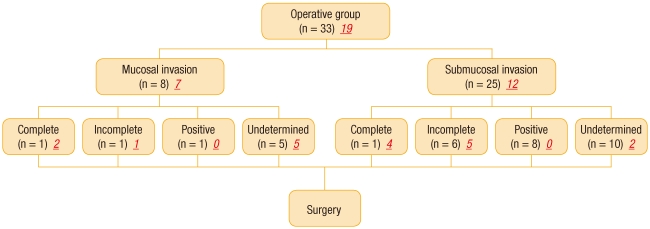
Methods: We examined the clinicopathologic characteristics, complications and prognoses among the patients who underwent a colonoscopic polypectomy in both our hospitals and at other hospitals from April 2003 and April 2010. These patients were divided into two groups, the group (non-operation group) that only underwent a polypectomy (n = 37) and the group (operation group) that underwent a polypectomy with subsequent surgery (n = 33).
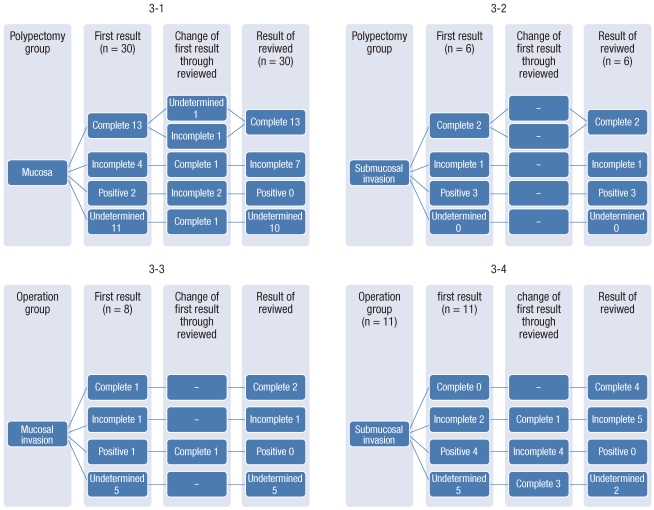
Results: There were no differences between two groups in the ratios of the number of men to the number of women, the ages or the comorbidities. In terms of endoscopic findings, we found no differences between the two groups in the locations of the polyps, the sizes of the polyps, or the presence of stalks. However, ulceration of polyps was higher in the non-operation group (51.5% vs. 21.6%; P = 0.009), as was the case with submucosal invasion (75.8% vs. 16.2%; P < 0.005). When an endoscopic polypectomy was performed, incomplete resection margins and specimens with margins involved occurred more frequently in the operation group (93.9% vs. 51.4%; P < 0.005), but no residual tumor was detected in 31 of 33 (93.9%) patients in that group. One pathologist reviewed the specimens of 54 patients (operation group, 19; non-operation group, 36). Six of the 19 polyps (31.6%) in the operation group and fifteen of the 36 polyps (41.7%) in the non-operation group had a margin without cancer cells.
Conclusion: We may accept the criterion of a safe margin, including a coagulation zone. A multidisciplinary approach has to be developed by surgeons, endoscopists and pathologists based on a discussion of the risk factors for the patient before making a decision on the treatment treatment.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
