Erika Khandor, Kate Mason, Catharine Chambers, Kate Rossiter, Laura Cowan, Stephen W Hwang
{"title":"加拿大多伦多无家可归成年人获得初级保健的情况:街头健康调查的结果。","authors":"Erika Khandor, Kate Mason, Catharine Chambers, Kate Rossiter, Laura Cowan, Stephen W Hwang","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite experiencing a disproportionate burden of acute and chronic health issues, many homeless people face barriers to primary health care. Most studies on health care access among homeless populations have been conducted in the United States, and relatively few are available from countries such as Canada that have a system of universal health insurance. We investigated access to primary health care among a representative sample of homeless adults in Toronto, Canada.</p><p><strong>Methods: </strong>Homeless adults were recruited from shelter and meal programs in downtown Toronto between November 2006 and February 2007. Cross-sectional data were collected on demographic characteristics, health status, health determinants and access to health care. We used multivariable logistic regression analysis to investigate the association between having a family doctor as the usual source of health care (an indicator of access to primary care) and health status, proof of health insurance, and substance use after adjustment for demographic characteristics.</p><p><strong>Results: </strong>Of the 366 participants included in our study, 156 (43%) reported having a family doctor. After adjustment for potential confounders and covariates, we found that the odds of having a family doctor significantly decreased with every additional year spent homeless in the participant's lifetime (adjusted odds ratio [OR] 0.91, 95% confidence interval [CI] 0.86-0.97). Having a family doctor was significantly associated with being lesbian, gay, bisexual or transgendered (adjusted OR 2.70, 95% CI 1.04-7.00), having a health card (proof of health insurance coverage in the province of Ontario) (adjusted OR 2.80, 95% CI 1.61-4.89) and having a chronic medical condition (adjusted OR 1.91, 95% CI 1.03-3.53).</p><p><strong>Interpretation: </strong>Less than half of the homeless people in Toronto who participated in our study reported having a family doctor. Not having a family doctor was associated with key indicators of health care access and health status, including increasing duration of homelessness, lack of proof of health insurance coverage and having a chronic medical condition. Increased efforts are needed to address the barriers to appropriate health care and good health that persist in this population despite the provision of health insurance.</p>","PeriodicalId":88624,"journal":{"name":"Open medicine : a peer-reviewed, independent, open-access journal","volume":"5 2","pages":"e94-e103"},"PeriodicalIF":0.0000,"publicationDate":"2011-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/45/01/OpenMed-05-e94.PMC3148004.pdf","citationCount":"0","resultStr":"{\"title\":\"Access to primary health care among homeless adults in Toronto, Canada: results from the Street Health survey.\",\"authors\":\"Erika Khandor, Kate Mason, Catharine Chambers, Kate Rossiter, Laura Cowan, Stephen W Hwang\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Despite experiencing a disproportionate burden of acute and chronic health issues, many homeless people face barriers to primary health care. Most studies on health care access among homeless populations have been conducted in the United States, and relatively few are available from countries such as Canada that have a system of universal health insurance. We investigated access to primary health care among a representative sample of homeless adults in Toronto, Canada.</p><p><strong>Methods: </strong>Homeless adults were recruited from shelter and meal programs in downtown Toronto between November 2006 and February 2007. Cross-sectional data were collected on demographic characteristics, health status, health determinants and access to health care. We used multivariable logistic regression analysis to investigate the association between having a family doctor as the usual source of health care (an indicator of access to primary care) and health status, proof of health insurance, and substance use after adjustment for demographic characteristics.</p><p><strong>Results: </strong>Of the 366 participants included in our study, 156 (43%) reported having a family doctor. After adjustment for potential confounders and covariates, we found that the odds of having a family doctor significantly decreased with every additional year spent homeless in the participant's lifetime (adjusted odds ratio [OR] 0.91, 95% confidence interval [CI] 0.86-0.97). Having a family doctor was significantly associated with being lesbian, gay, bisexual or transgendered (adjusted OR 2.70, 95% CI 1.04-7.00), having a health card (proof of health insurance coverage in the province of Ontario) (adjusted OR 2.80, 95% CI 1.61-4.89) and having a chronic medical condition (adjusted OR 1.91, 95% CI 1.03-3.53).</p><p><strong>Interpretation: </strong>Less than half of the homeless people in Toronto who participated in our study reported having a family doctor. Not having a family doctor was associated with key indicators of health care access and health status, including increasing duration of homelessness, lack of proof of health insurance coverage and having a chronic medical condition. Increased efforts are needed to address the barriers to appropriate health care and good health that persist in this population despite the provision of health insurance.</p>\",\"PeriodicalId\":88624,\"journal\":{\"name\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"volume\":\"5 2\",\"pages\":\"e94-e103\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/45/01/OpenMed-05-e94.PMC3148004.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open medicine : a peer-reviewed, independent, open-access journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2011/5/24 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open medicine : a peer-reviewed, independent, open-access journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2011/5/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Access to primary health care among homeless adults in Toronto, Canada: results from the Street Health survey.
Background: Despite experiencing a disproportionate burden of acute and chronic health issues, many homeless people face barriers to primary health care. Most studies on health care access among homeless populations have been conducted in the United States, and relatively few are available from countries such as Canada that have a system of universal health insurance. We investigated access to primary health care among a representative sample of homeless adults in Toronto, Canada.
Methods: Homeless adults were recruited from shelter and meal programs in downtown Toronto between November 2006 and February 2007. Cross-sectional data were collected on demographic characteristics, health status, health determinants and access to health care. We used multivariable logistic regression analysis to investigate the association between having a family doctor as the usual source of health care (an indicator of access to primary care) and health status, proof of health insurance, and substance use after adjustment for demographic characteristics.
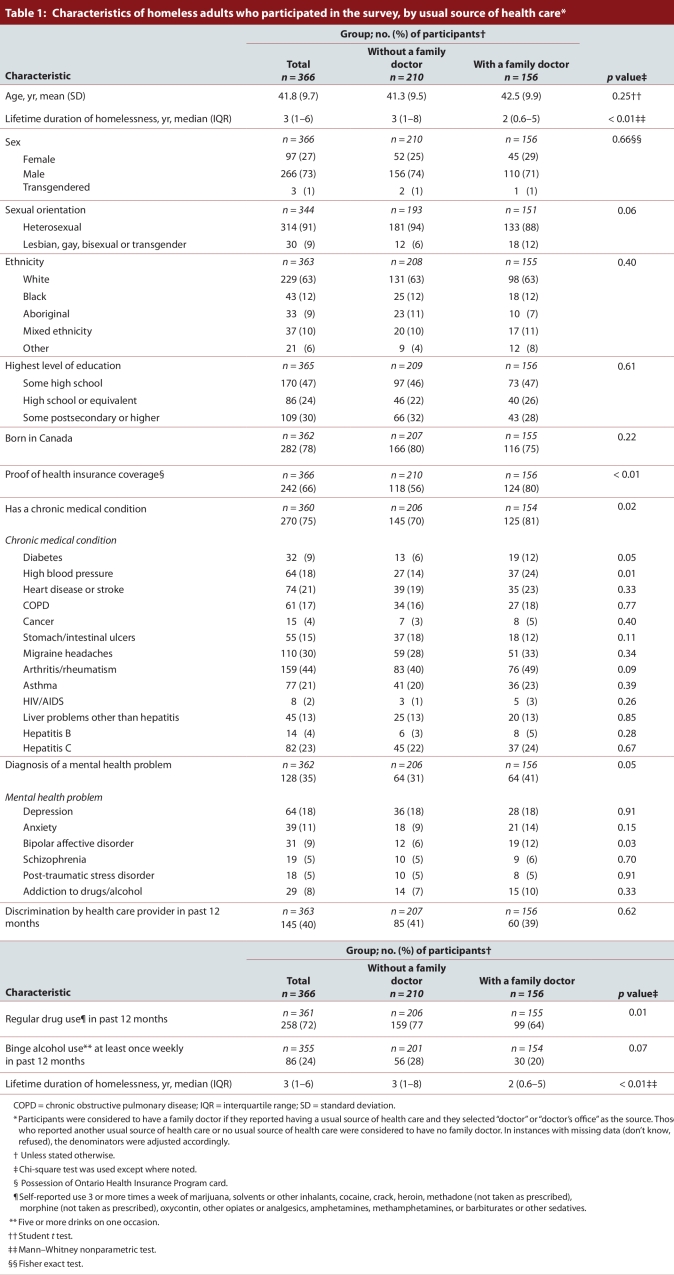
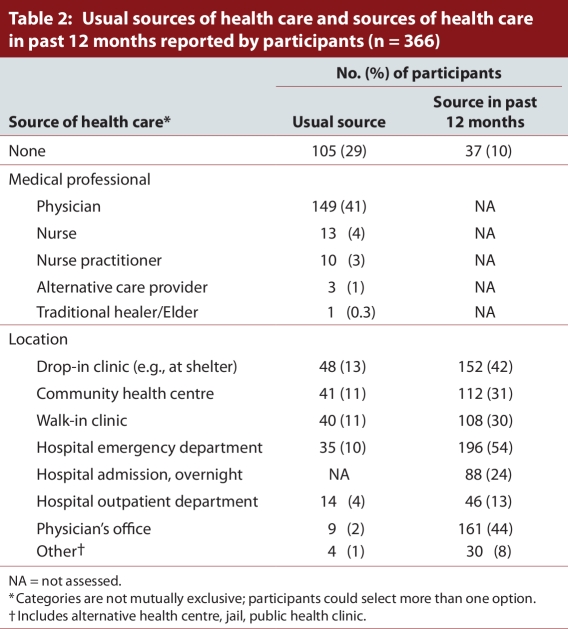
Results: Of the 366 participants included in our study, 156 (43%) reported having a family doctor. After adjustment for potential confounders and covariates, we found that the odds of having a family doctor significantly decreased with every additional year spent homeless in the participant's lifetime (adjusted odds ratio [OR] 0.91, 95% confidence interval [CI] 0.86-0.97). Having a family doctor was significantly associated with being lesbian, gay, bisexual or transgendered (adjusted OR 2.70, 95% CI 1.04-7.00), having a health card (proof of health insurance coverage in the province of Ontario) (adjusted OR 2.80, 95% CI 1.61-4.89) and having a chronic medical condition (adjusted OR 1.91, 95% CI 1.03-3.53).
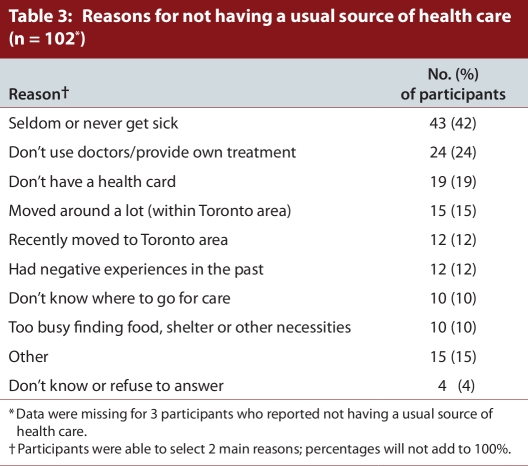
Interpretation: Less than half of the homeless people in Toronto who participated in our study reported having a family doctor. Not having a family doctor was associated with key indicators of health care access and health status, including increasing duration of homelessness, lack of proof of health insurance coverage and having a chronic medical condition. Increased efforts are needed to address the barriers to appropriate health care and good health that persist in this population despite the provision of health insurance.
 分享
分享




 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
