R Christian Crumrine, Victor J Marder, G McLeod Taylor, Joseph C Lamanna, Constantinos P Tsipis, Philip Scuderi, Stephen R Petteway, Vikram Arora
{"title":"重组组织型纤溶酶原激活剂(rt-PA)在短暂性大鼠大脑中动脉闭塞模型中引起比静脉注射rt-PA更多的颅内出血。","authors":"R Christian Crumrine, Victor J Marder, G McLeod Taylor, Joseph C Lamanna, Constantinos P Tsipis, Philip Scuderi, Stephen R Petteway, Vikram Arora","doi":"10.1186/2040-7378-3-10","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Intra-arterial (IA) administration of rt-PA for ischemic stroke has the potential for greater thrombolytic efficacy, especially for a large thrombus in the M1 or M2 segment of the middle cerebral artery (MCA). Intracranial hemorrhage (ICH) is a concern with IA or intravenous (IV) administration especially as the therapeutic window is extended. However, because IA administration delivers a higher local concentration of agent, the incidence and severity of ICH may be greater than with similar doses IV. We investigated the safety of rt-PA administration by IA compared to IV infusion following 6 hours of MCA occlusion (MCAo) with reflow in the spontaneously hypertensive rat (SHR).</p><p><strong>Methods: </strong>Male SHRs were subjected to 6 hours MCAo with 18 hours reflow using a snare ligature model. They were treated with IA saline, IA rt-PA (1, 5, 10, 30 mg/kg), or IV rt-PA (10 and 30 mg/kg) by a 10 to 60 minute infusion beginning approximately 1 minute before reflow. The rats were recovered for 24 hours after MCAo onset at which time Bleeding Score, infarct volume, and Modified Bederson Score were measured.</p><p><strong>Results: </strong>Greater hemorrhagic transformation occurred with 10 and 30 mg/kg rt-PA administered IA than IV. The IV 10 mg/kg rt-PA dosage induced significantly less bleeding than did the 1 or 5 mg/kg IA groups. No significant increase in infarct volume was observed after IA or IV treatment. Rats treated with 30 mg/kg rt-PA by either the IA or IV route had greater neurological dysfunction compared to all other groups.</p><p><strong>Conclusions: </strong>Administration of rt-PA by the IA route following 6 hours of MCAo results in greater ICH and worse functional recovery than comparable dosages IV. Significantly greater bleeding was observed when the IA dose was a tenth of the IV dose. The increased bleeding did not translate in larger infarct volumes.</p>","PeriodicalId":12158,"journal":{"name":"Experimental & Translational Stroke Medicine","volume":"3 1","pages":"10"},"PeriodicalIF":0.0000,"publicationDate":"2011-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/2040-7378-3-10","citationCount":"18","resultStr":"{\"title\":\"Intra-arterial administration of recombinant tissue-type plasminogen activator (rt-PA) causes more intracranial bleeding than does intravenous rt-PA in a transient rat middle cerebral artery occlusion model.\",\"authors\":\"R Christian Crumrine, Victor J Marder, G McLeod Taylor, Joseph C Lamanna, Constantinos P Tsipis, Philip Scuderi, Stephen R Petteway, Vikram Arora\",\"doi\":\"10.1186/2040-7378-3-10\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Intra-arterial (IA) administration of rt-PA for ischemic stroke has the potential for greater thrombolytic efficacy, especially for a large thrombus in the M1 or M2 segment of the middle cerebral artery (MCA). Intracranial hemorrhage (ICH) is a concern with IA or intravenous (IV) administration especially as the therapeutic window is extended. However, because IA administration delivers a higher local concentration of agent, the incidence and severity of ICH may be greater than with similar doses IV. We investigated the safety of rt-PA administration by IA compared to IV infusion following 6 hours of MCA occlusion (MCAo) with reflow in the spontaneously hypertensive rat (SHR).</p><p><strong>Methods: </strong>Male SHRs were subjected to 6 hours MCAo with 18 hours reflow using a snare ligature model. They were treated with IA saline, IA rt-PA (1, 5, 10, 30 mg/kg), or IV rt-PA (10 and 30 mg/kg) by a 10 to 60 minute infusion beginning approximately 1 minute before reflow. The rats were recovered for 24 hours after MCAo onset at which time Bleeding Score, infarct volume, and Modified Bederson Score were measured.</p><p><strong>Results: </strong>Greater hemorrhagic transformation occurred with 10 and 30 mg/kg rt-PA administered IA than IV. The IV 10 mg/kg rt-PA dosage induced significantly less bleeding than did the 1 or 5 mg/kg IA groups. No significant increase in infarct volume was observed after IA or IV treatment. Rats treated with 30 mg/kg rt-PA by either the IA or IV route had greater neurological dysfunction compared to all other groups.</p><p><strong>Conclusions: </strong>Administration of rt-PA by the IA route following 6 hours of MCAo results in greater ICH and worse functional recovery than comparable dosages IV. Significantly greater bleeding was observed when the IA dose was a tenth of the IV dose. The increased bleeding did not translate in larger infarct volumes.</p>\",\"PeriodicalId\":12158,\"journal\":{\"name\":\"Experimental & Translational Stroke Medicine\",\"volume\":\"3 1\",\"pages\":\"10\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-09-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/2040-7378-3-10\",\"citationCount\":\"18\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Experimental & Translational Stroke Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/2040-7378-3-10\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Experimental & Translational Stroke Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/2040-7378-3-10","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Intra-arterial administration of recombinant tissue-type plasminogen activator (rt-PA) causes more intracranial bleeding than does intravenous rt-PA in a transient rat middle cerebral artery occlusion model.
Background: Intra-arterial (IA) administration of rt-PA for ischemic stroke has the potential for greater thrombolytic efficacy, especially for a large thrombus in the M1 or M2 segment of the middle cerebral artery (MCA). Intracranial hemorrhage (ICH) is a concern with IA or intravenous (IV) administration especially as the therapeutic window is extended. However, because IA administration delivers a higher local concentration of agent, the incidence and severity of ICH may be greater than with similar doses IV. We investigated the safety of rt-PA administration by IA compared to IV infusion following 6 hours of MCA occlusion (MCAo) with reflow in the spontaneously hypertensive rat (SHR).
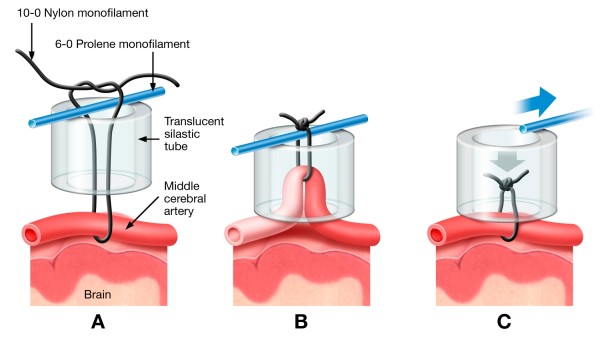
Methods: Male SHRs were subjected to 6 hours MCAo with 18 hours reflow using a snare ligature model. They were treated with IA saline, IA rt-PA (1, 5, 10, 30 mg/kg), or IV rt-PA (10 and 30 mg/kg) by a 10 to 60 minute infusion beginning approximately 1 minute before reflow. The rats were recovered for 24 hours after MCAo onset at which time Bleeding Score, infarct volume, and Modified Bederson Score were measured.
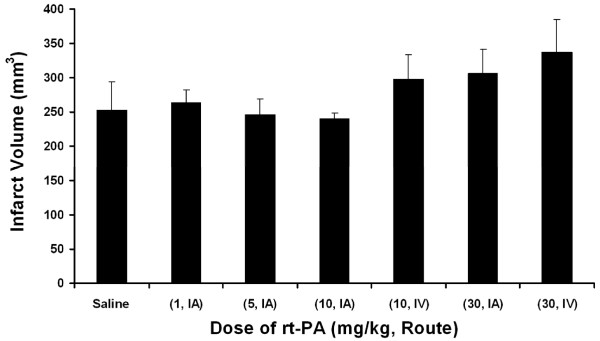
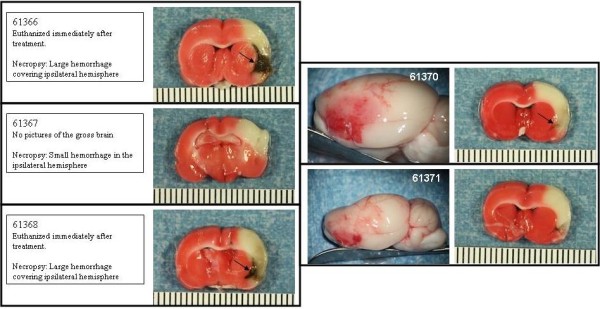
Results: Greater hemorrhagic transformation occurred with 10 and 30 mg/kg rt-PA administered IA than IV. The IV 10 mg/kg rt-PA dosage induced significantly less bleeding than did the 1 or 5 mg/kg IA groups. No significant increase in infarct volume was observed after IA or IV treatment. Rats treated with 30 mg/kg rt-PA by either the IA or IV route had greater neurological dysfunction compared to all other groups.
Conclusions: Administration of rt-PA by the IA route following 6 hours of MCAo results in greater ICH and worse functional recovery than comparable dosages IV. Significantly greater bleeding was observed when the IA dose was a tenth of the IV dose. The increased bleeding did not translate in larger infarct volumes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
