Jin Seong Cho, Sun Hyoung Shin, Young Ju Song, Hee Kyung Kim, Min Ho Park, Jung Han Yoon, Young Jong Jegal
{"title":"是否可以通过促甲状腺素、甲状腺球蛋白、抗甲状腺球蛋白和抗微粒体抗体来预测甲状腺切除术后甲状腺功能减退?","authors":"Jin Seong Cho, Sun Hyoung Shin, Young Ju Song, Hee Kyung Kim, Min Ho Park, Jung Han Yoon, Young Jong Jegal","doi":"10.4174/jkss.2011.81.6.380","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We investigated the incidence and risk factors of hypothyroidism after thyroid lobectomy, and evaluated the possibility to predict hypothyroidism preoperatively with serologic markers, such as thyrotropin (TSH), thyroglobulin (TG), anti-thyroglobulin (ATA), and anti-microsomal antibody (AMA).</p><p><strong>Methods: </strong>We enrolled 123 consecutive patients who underwent thyroid lobectomy due to benign conditions between May 2004 and April 2008. Only preoperative euthyroid patients were included. Patients were divided into two groups by postoperative thyroid function outcomes, into hypothyroid (n = 97) and euthyroid groups (n = 26), and analyzed specially for the preoperative levels of TSH, TG, ATA, and AMA.</p><p><strong>Results: </strong>Twenty-six (21.1%) patients developed hypothyroidism following thyroid lobectomy within 35.7 months of follow-up. The proportion of post-lobectomy hypothyroidism was high in patients with high-normal preoperative TSH level, and the cut-off value was 2.0 mIU/L, with 67% sensitivity and 75% specificity. The quantitative titer of preoperative TG, ATA, and AMA was not significant, but the outcome of categorical analysis of two or more positivities on these three markers was significantly higher in hypothyroid patients than in euthyroid patients (28.6% vs. 3.9%, P = 0.024). The combined positivity of preoperative TSH and two or more positivities of TG, ATA, and AMA possess 100% positive predictive value and 81% negative predictive value.</p><p><strong>Conclusion: </strong>The incidence of hypothyroidism following thyroid lobectomy was 21.1%. High-normal preoperative TSH and two or more positivities for TG, ATA, and AMA are good pre-operative predictive markers. Such high-risk patients need close TSH monitoring before the onset of clinical hypothyroidism.</p>","PeriodicalId":49157,"journal":{"name":"Journal of the Korean Surgical Society","volume":"81 6","pages":"380-6"},"PeriodicalIF":0.0000,"publicationDate":"2011-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4174/jkss.2011.81.6.380","citationCount":"19","resultStr":"{\"title\":\"Is it possible to predict hypothyroidism after thyroid lobectomy through thyrotropin, thyroglobulin, anti-thyroglobulin, and anti-microsomal antibody?\",\"authors\":\"Jin Seong Cho, Sun Hyoung Shin, Young Ju Song, Hee Kyung Kim, Min Ho Park, Jung Han Yoon, Young Jong Jegal\",\"doi\":\"10.4174/jkss.2011.81.6.380\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>We investigated the incidence and risk factors of hypothyroidism after thyroid lobectomy, and evaluated the possibility to predict hypothyroidism preoperatively with serologic markers, such as thyrotropin (TSH), thyroglobulin (TG), anti-thyroglobulin (ATA), and anti-microsomal antibody (AMA).</p><p><strong>Methods: </strong>We enrolled 123 consecutive patients who underwent thyroid lobectomy due to benign conditions between May 2004 and April 2008. Only preoperative euthyroid patients were included. Patients were divided into two groups by postoperative thyroid function outcomes, into hypothyroid (n = 97) and euthyroid groups (n = 26), and analyzed specially for the preoperative levels of TSH, TG, ATA, and AMA.</p><p><strong>Results: </strong>Twenty-six (21.1%) patients developed hypothyroidism following thyroid lobectomy within 35.7 months of follow-up. The proportion of post-lobectomy hypothyroidism was high in patients with high-normal preoperative TSH level, and the cut-off value was 2.0 mIU/L, with 67% sensitivity and 75% specificity. The quantitative titer of preoperative TG, ATA, and AMA was not significant, but the outcome of categorical analysis of two or more positivities on these three markers was significantly higher in hypothyroid patients than in euthyroid patients (28.6% vs. 3.9%, P = 0.024). The combined positivity of preoperative TSH and two or more positivities of TG, ATA, and AMA possess 100% positive predictive value and 81% negative predictive value.</p><p><strong>Conclusion: </strong>The incidence of hypothyroidism following thyroid lobectomy was 21.1%. High-normal preoperative TSH and two or more positivities for TG, ATA, and AMA are good pre-operative predictive markers. Such high-risk patients need close TSH monitoring before the onset of clinical hypothyroidism.</p>\",\"PeriodicalId\":49157,\"journal\":{\"name\":\"Journal of the Korean Surgical Society\",\"volume\":\"81 6\",\"pages\":\"380-6\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.4174/jkss.2011.81.6.380\",\"citationCount\":\"19\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Korean Surgical Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4174/jkss.2011.81.6.380\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2011/11/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Korean Surgical Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4174/jkss.2011.81.6.380","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2011/11/25 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 19
摘要
目的:探讨甲状腺小叶切除术后甲状腺功能减退的发生率及危险因素,并评估术前血清指标如促甲状腺素(TSH)、甲状腺球蛋白(TG)、抗甲状腺球蛋白(ATA)、抗微粒体抗体(AMA)预测甲状腺功能减退的可能性。方法:在2004年5月至2008年4月期间,我们招募了123例因良性疾病而接受甲状腺小叶切除术的患者。仅纳入术前甲状腺功能正常的患者。根据术后甲状腺功能情况将患者分为两组,分别为甲状腺功能低下组(n = 97)和甲状腺功能正常组(n = 26),特别分析术前TSH、TG、ATA、AMA水平。结果:随访35.7个月,甲状腺小叶切除术后发生甲状腺功能减退26例(21.1%)。术前TSH水平高正常的患者,肺叶切除术后甲状腺功能减退的比例较高,临界值为2.0 mIU/L,敏感性67%,特异性75%。术前TG、ATA、AMA的定量滴度无统计学意义,但甲状腺功能减退患者两项及两项以上指标阳性的分类分析结果明显高于甲状腺功能正常患者(28.6% vs. 3.9%, P = 0.024)。术前TSH阳性与TG、ATA、AMA两项或两项以上阳性联合,阳性预测值为100%,阴性预测值为81%。结论:甲状腺小叶切除术后甲状腺功能减退的发生率为21.1%。术前高正常TSH和两项或两项以上TG、ATA和AMA阳性是良好的术前预测指标。这类高危患者在临床甲状腺功能减退发病前需要密切监测TSH。
Is it possible to predict hypothyroidism after thyroid lobectomy through thyrotropin, thyroglobulin, anti-thyroglobulin, and anti-microsomal antibody?
Purpose: We investigated the incidence and risk factors of hypothyroidism after thyroid lobectomy, and evaluated the possibility to predict hypothyroidism preoperatively with serologic markers, such as thyrotropin (TSH), thyroglobulin (TG), anti-thyroglobulin (ATA), and anti-microsomal antibody (AMA).
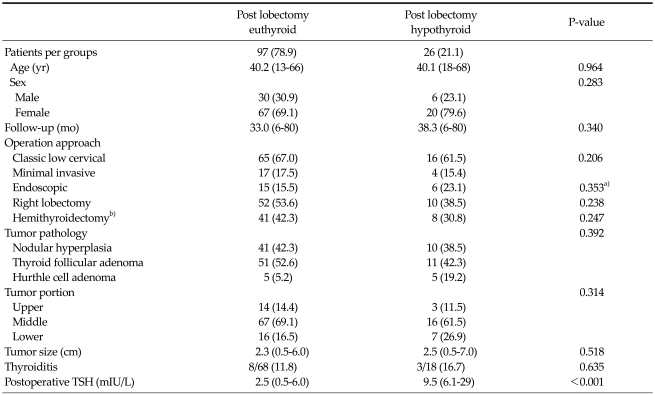
Methods: We enrolled 123 consecutive patients who underwent thyroid lobectomy due to benign conditions between May 2004 and April 2008. Only preoperative euthyroid patients were included. Patients were divided into two groups by postoperative thyroid function outcomes, into hypothyroid (n = 97) and euthyroid groups (n = 26), and analyzed specially for the preoperative levels of TSH, TG, ATA, and AMA.
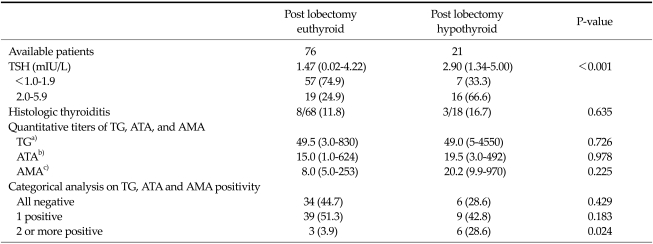
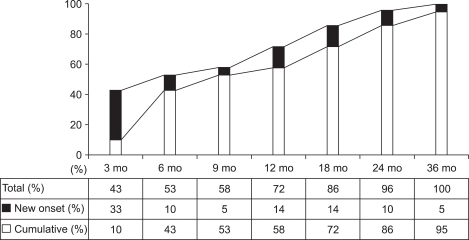
Results: Twenty-six (21.1%) patients developed hypothyroidism following thyroid lobectomy within 35.7 months of follow-up. The proportion of post-lobectomy hypothyroidism was high in patients with high-normal preoperative TSH level, and the cut-off value was 2.0 mIU/L, with 67% sensitivity and 75% specificity. The quantitative titer of preoperative TG, ATA, and AMA was not significant, but the outcome of categorical analysis of two or more positivities on these three markers was significantly higher in hypothyroid patients than in euthyroid patients (28.6% vs. 3.9%, P = 0.024). The combined positivity of preoperative TSH and two or more positivities of TG, ATA, and AMA possess 100% positive predictive value and 81% negative predictive value.
Conclusion: The incidence of hypothyroidism following thyroid lobectomy was 21.1%. High-normal preoperative TSH and two or more positivities for TG, ATA, and AMA are good pre-operative predictive markers. Such high-risk patients need close TSH monitoring before the onset of clinical hypothyroidism.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
