Debasish Banerjee, Allan J Collins, Charles A Herzog
{"title":"炎症对血液透析患者脉压与死亡率关系的影响。","authors":"Debasish Banerjee, Allan J Collins, Charles A Herzog","doi":"10.1159/000335691","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aim: </strong>The effect of hypertension on mortality in haemodialysis patients is controversial and can be confounded by non-traditional risk factors like systemic inflammation. This study examined the effect of systolic blood pressure (SBP), diastolic blood pressure (DBP), and pulse pressure (PP) on mortality in haemodialysis patients, separately with and without markers of systemic inflammation.</p><p><strong>Methods: </strong>Data from the United States Renal Data System were analysed for 9,862 patients receiving haemodialysis on December 31, 1993, followed through May 2005.</p><p><strong>Results: </strong>In Cox regression analysis, increased age, diabetes, low albumin, high white blood count, low cholesterol, low haemoglobin, high phosphate, low DBP, and cardiovascular comorbidity were associated with high mortality, but SBP was not. Elevated PP adjusted for SBP, age, diabetes, haemoglobin, albumin, cholesterol, calcium, phosphate, parathyroid hormone, and white blood count was associated with higher mortality [adjusted hazard ratio, PP 1.006 (95% confidence interval, CI, 1.002-1.010); SBP 0.993 (95% CI 0.990-0.996)]. In dual models, PP adjusted for SBP then DBP was associated with higher mortality [PP 1.029 (95% CI 1.027-1.032); SBP 0.981 (95% CI 0.979-0.983); PP 1.010 (95% CI 1.008-1.011); DBP 0.981 (95% CI 0.979-0.983)]. Increasing PP deciles >70 mm Hg were associated with increasing mortality in the absence of markers of systemic inflammation (white blood count >10 × 10(9)/l, albumin <3.5 g/dl, diabetes), but not in their presence.</p><p><strong>Conclusion: </strong>PP was a better indicator of adverse outcome than DBP or SBP. Inflammation-associated injury may mask the effect of PP on mortality in haemodialysis patients.</p>","PeriodicalId":56356,"journal":{"name":"Nephron Extra","volume":"1 1","pages":"292-9"},"PeriodicalIF":0.0000,"publicationDate":"2011-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000335691","citationCount":"1","resultStr":"{\"title\":\"Effect of inflammation on the relationship of pulse pressure and mortality in haemodialysis.\",\"authors\":\"Debasish Banerjee, Allan J Collins, Charles A Herzog\",\"doi\":\"10.1159/000335691\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background/aim: </strong>The effect of hypertension on mortality in haemodialysis patients is controversial and can be confounded by non-traditional risk factors like systemic inflammation. This study examined the effect of systolic blood pressure (SBP), diastolic blood pressure (DBP), and pulse pressure (PP) on mortality in haemodialysis patients, separately with and without markers of systemic inflammation.</p><p><strong>Methods: </strong>Data from the United States Renal Data System were analysed for 9,862 patients receiving haemodialysis on December 31, 1993, followed through May 2005.</p><p><strong>Results: </strong>In Cox regression analysis, increased age, diabetes, low albumin, high white blood count, low cholesterol, low haemoglobin, high phosphate, low DBP, and cardiovascular comorbidity were associated with high mortality, but SBP was not. Elevated PP adjusted for SBP, age, diabetes, haemoglobin, albumin, cholesterol, calcium, phosphate, parathyroid hormone, and white blood count was associated with higher mortality [adjusted hazard ratio, PP 1.006 (95% confidence interval, CI, 1.002-1.010); SBP 0.993 (95% CI 0.990-0.996)]. In dual models, PP adjusted for SBP then DBP was associated with higher mortality [PP 1.029 (95% CI 1.027-1.032); SBP 0.981 (95% CI 0.979-0.983); PP 1.010 (95% CI 1.008-1.011); DBP 0.981 (95% CI 0.979-0.983)]. Increasing PP deciles >70 mm Hg were associated with increasing mortality in the absence of markers of systemic inflammation (white blood count >10 × 10(9)/l, albumin <3.5 g/dl, diabetes), but not in their presence.</p><p><strong>Conclusion: </strong>PP was a better indicator of adverse outcome than DBP or SBP. Inflammation-associated injury may mask the effect of PP on mortality in haemodialysis patients.</p>\",\"PeriodicalId\":56356,\"journal\":{\"name\":\"Nephron Extra\",\"volume\":\"1 1\",\"pages\":\"292-9\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1159/000335691\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nephron Extra\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000335691\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2012/1/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nephron Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000335691","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/1/18 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
背景/目的:高血压对血液透析患者死亡率的影响是有争议的,可能与全身性炎症等非传统危险因素相混淆。本研究分别检测了收缩压(SBP)、舒张压(DBP)和脉压(PP)对血液透析患者死亡率的影响,有和没有全身性炎症标志物。方法:对1993年12月31日至2005年5月接受血液透析的9862例患者的美国肾脏数据系统数据进行分析。结果:在Cox回归分析中,年龄增加、糖尿病、低白蛋白、高白细胞计数、低胆固醇、低血红蛋白、高磷酸盐、低舒张压和心血管合并症与高死亡率相关,但收缩压无关。经收缩压、年龄、糖尿病、血红蛋白、白蛋白、胆固醇、钙、磷酸盐、甲状旁腺激素和白细胞计数校正的PP升高与较高的死亡率相关[校正风险比,PP 1.006(95%可信区间,CI 1.002-1.010);SBP 0.993 (95% ci 0.990-0.996)]。在双重模型中,经收缩压和舒张压校正的PP与较高的死亡率相关[PP 1.029 (95% CI 1.027-1.032);SBP 0.981 (95% ci 0.979-0.983);Pp 1.010 (95% ci 1.008-1.011);DBP 0.981 (95% ci 0.979-0.983)]。在没有全身性炎症标志物(白细胞计数>10 × 10(9)/l,白蛋白)的情况下,PP升高>70 mm Hg与死亡率升高相关。结论:PP是比舒张压或收缩压更好的不良结局指标。炎症相关损伤可能掩盖PP对血液透析患者死亡率的影响。
Effect of inflammation on the relationship of pulse pressure and mortality in haemodialysis.
Background/aim: The effect of hypertension on mortality in haemodialysis patients is controversial and can be confounded by non-traditional risk factors like systemic inflammation. This study examined the effect of systolic blood pressure (SBP), diastolic blood pressure (DBP), and pulse pressure (PP) on mortality in haemodialysis patients, separately with and without markers of systemic inflammation.
Methods: Data from the United States Renal Data System were analysed for 9,862 patients receiving haemodialysis on December 31, 1993, followed through May 2005.
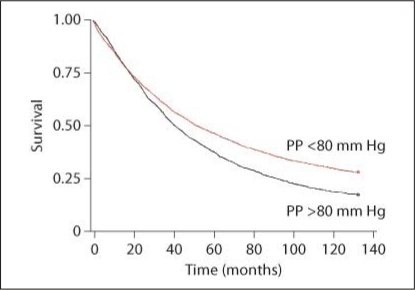
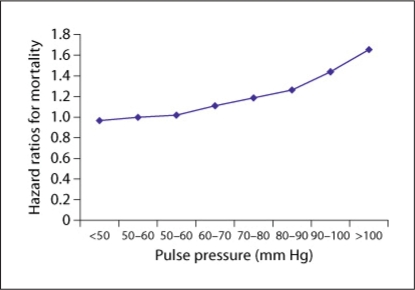
Results: In Cox regression analysis, increased age, diabetes, low albumin, high white blood count, low cholesterol, low haemoglobin, high phosphate, low DBP, and cardiovascular comorbidity were associated with high mortality, but SBP was not. Elevated PP adjusted for SBP, age, diabetes, haemoglobin, albumin, cholesterol, calcium, phosphate, parathyroid hormone, and white blood count was associated with higher mortality [adjusted hazard ratio, PP 1.006 (95% confidence interval, CI, 1.002-1.010); SBP 0.993 (95% CI 0.990-0.996)]. In dual models, PP adjusted for SBP then DBP was associated with higher mortality [PP 1.029 (95% CI 1.027-1.032); SBP 0.981 (95% CI 0.979-0.983); PP 1.010 (95% CI 1.008-1.011); DBP 0.981 (95% CI 0.979-0.983)]. Increasing PP deciles >70 mm Hg were associated with increasing mortality in the absence of markers of systemic inflammation (white blood count >10 × 10(9)/l, albumin <3.5 g/dl, diabetes), but not in their presence.
Conclusion: PP was a better indicator of adverse outcome than DBP or SBP. Inflammation-associated injury may mask the effect of PP on mortality in haemodialysis patients.
期刊介绍:
An open-access subjournal to Nephron. ''Nephron EXTRA'' publishes additional high-quality articles that cannot be published in the main journal ''Nephron'' due to space limitations.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
