Hong Yeol Yoo, Rumi Shin, Heon-Kyun Ha, Heung-Kwon Oh, Seung-Yong Jeong, Kyu Joo Park, Gyeong Hoon Kang, Woo Ho Kim, Jae-Gahb Park
{"title":"t3细分与结直肠癌淋巴结或远处转移相关吗?","authors":"Hong Yeol Yoo, Rumi Shin, Heon-Kyun Ha, Heung-Kwon Oh, Seung-Yong Jeong, Kyu Joo Park, Gyeong Hoon Kang, Woo Ho Kim, Jae-Gahb Park","doi":"10.3393/jksc.2012.28.3.160","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We analyzed the clinical data of T3 colorectal cancer patients to assess whether T3 subdivision correlates with node (N) or metastasis (M) staging and stage-independent factors.</p><p><strong>Methods: </strong>Five hundred fifty-five patients who underwent surgery for primary colorectal cancer from January 2003 to December 2009 were analyzed for T3 subdivision. T3 subdivision was determined by the depth of invasion beyond the outer border of the proper muscle (T3a, <1 mm; T3b, 1 to 5 mm; T3c, >5 to 15 mm; T3d, >15 mm). We investigated the correlation between T3 subdivision and N, M staging and stage-independent prognostic factors including angiolymphatic invasion (ALI), venous invasion (VI) and perineural invasion (PNI).</p><p><strong>Results: </strong>The tumors of the 555 patients were subclassified as T3a in 86 patients (15.5%), T3b in 209 patients (37.7%), T3c in 210 patients (37.8%) and T3d in 50 patients (9.0%). The nodal metastasis rates were 39.5% for T3a, 56.5% for T3b, 75.7% for T3c and 74.0% for T3d. The distant metastasis rates were 7.0% for T3a 9.1% for T3b, 27.1% for T3c and 40.0% for T3d. Both N and M staging correlated with T3 subdivision (Spearman's rho = 0.288, 0.276, respectively; P < 0.001). Other stage-independent prognostic factors correlated well with T3 subdivision (Spearman's rho = 0.250, P < 0.001 for ALI; rho = 0.146, P < 0.001 for VI; rho = 0.271, P < 0.001 for PNI).</p><p><strong>Conclusion: </strong>Subdivision of T3 colorectal cancer correlates with nodal and metastasis staging. Moreover, it correlates with other prognostic factors for colorectal cancer.</p>","PeriodicalId":17346,"journal":{"name":"Journal of the Korean Society of Coloproctology","volume":null,"pages":null},"PeriodicalIF":0.0000,"publicationDate":"2012-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a8/61/jksc-28-160.PMC3398112.pdf","citationCount":"12","resultStr":"{\"title\":\"Does t3 subdivision correlate with nodal or distant metastasis in colorectal cancer?\",\"authors\":\"Hong Yeol Yoo, Rumi Shin, Heon-Kyun Ha, Heung-Kwon Oh, Seung-Yong Jeong, Kyu Joo Park, Gyeong Hoon Kang, Woo Ho Kim, Jae-Gahb Park\",\"doi\":\"10.3393/jksc.2012.28.3.160\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>We analyzed the clinical data of T3 colorectal cancer patients to assess whether T3 subdivision correlates with node (N) or metastasis (M) staging and stage-independent factors.</p><p><strong>Methods: </strong>Five hundred fifty-five patients who underwent surgery for primary colorectal cancer from January 2003 to December 2009 were analyzed for T3 subdivision. T3 subdivision was determined by the depth of invasion beyond the outer border of the proper muscle (T3a, <1 mm; T3b, 1 to 5 mm; T3c, >5 to 15 mm; T3d, >15 mm). We investigated the correlation between T3 subdivision and N, M staging and stage-independent prognostic factors including angiolymphatic invasion (ALI), venous invasion (VI) and perineural invasion (PNI).</p><p><strong>Results: </strong>The tumors of the 555 patients were subclassified as T3a in 86 patients (15.5%), T3b in 209 patients (37.7%), T3c in 210 patients (37.8%) and T3d in 50 patients (9.0%). The nodal metastasis rates were 39.5% for T3a, 56.5% for T3b, 75.7% for T3c and 74.0% for T3d. The distant metastasis rates were 7.0% for T3a 9.1% for T3b, 27.1% for T3c and 40.0% for T3d. Both N and M staging correlated with T3 subdivision (Spearman's rho = 0.288, 0.276, respectively; P < 0.001). Other stage-independent prognostic factors correlated well with T3 subdivision (Spearman's rho = 0.250, P < 0.001 for ALI; rho = 0.146, P < 0.001 for VI; rho = 0.271, P < 0.001 for PNI).</p><p><strong>Conclusion: </strong>Subdivision of T3 colorectal cancer correlates with nodal and metastasis staging. Moreover, it correlates with other prognostic factors for colorectal cancer.</p>\",\"PeriodicalId\":17346,\"journal\":{\"name\":\"Journal of the Korean Society of Coloproctology\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2012-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a8/61/jksc-28-160.PMC3398112.pdf\",\"citationCount\":\"12\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Korean Society of Coloproctology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3393/jksc.2012.28.3.160\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2012/6/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Korean Society of Coloproctology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3393/jksc.2012.28.3.160","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/6/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Does t3 subdivision correlate with nodal or distant metastasis in colorectal cancer?
Purpose: We analyzed the clinical data of T3 colorectal cancer patients to assess whether T3 subdivision correlates with node (N) or metastasis (M) staging and stage-independent factors.
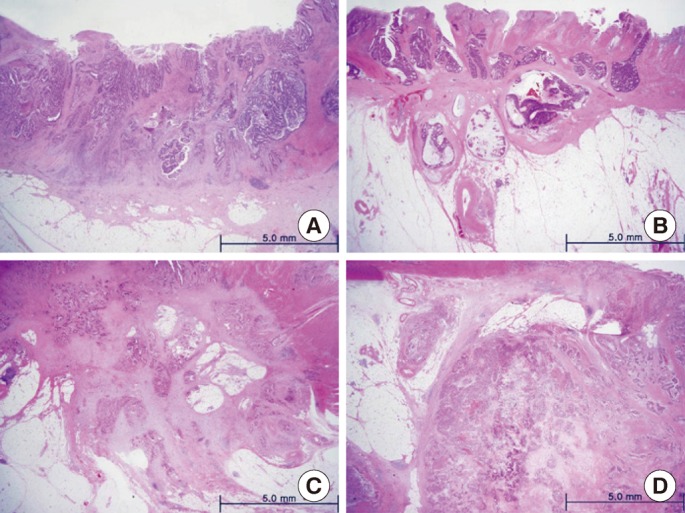
Methods: Five hundred fifty-five patients who underwent surgery for primary colorectal cancer from January 2003 to December 2009 were analyzed for T3 subdivision. T3 subdivision was determined by the depth of invasion beyond the outer border of the proper muscle (T3a, <1 mm; T3b, 1 to 5 mm; T3c, >5 to 15 mm; T3d, >15 mm). We investigated the correlation between T3 subdivision and N, M staging and stage-independent prognostic factors including angiolymphatic invasion (ALI), venous invasion (VI) and perineural invasion (PNI).
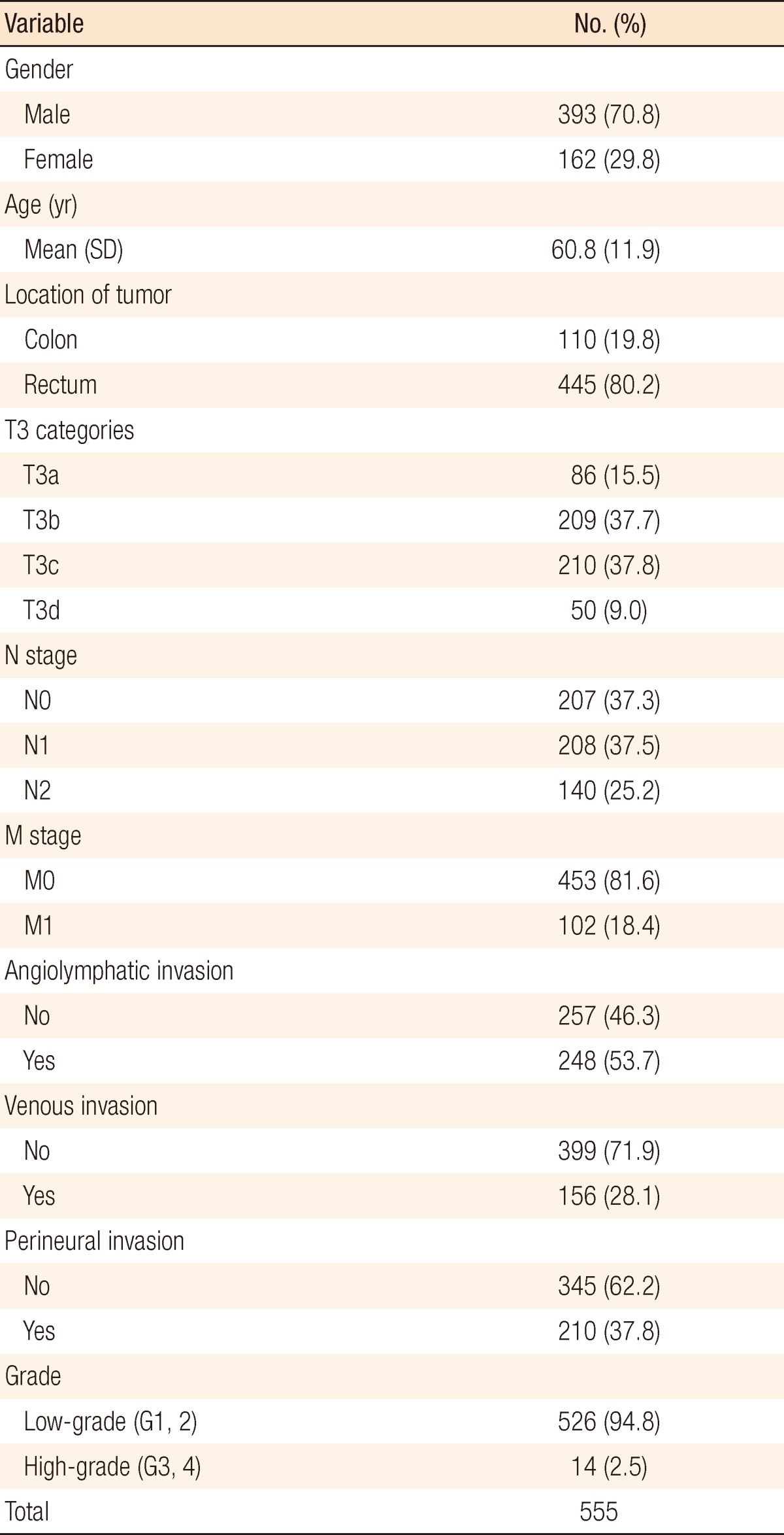
Results: The tumors of the 555 patients were subclassified as T3a in 86 patients (15.5%), T3b in 209 patients (37.7%), T3c in 210 patients (37.8%) and T3d in 50 patients (9.0%). The nodal metastasis rates were 39.5% for T3a, 56.5% for T3b, 75.7% for T3c and 74.0% for T3d. The distant metastasis rates were 7.0% for T3a 9.1% for T3b, 27.1% for T3c and 40.0% for T3d. Both N and M staging correlated with T3 subdivision (Spearman's rho = 0.288, 0.276, respectively; P < 0.001). Other stage-independent prognostic factors correlated well with T3 subdivision (Spearman's rho = 0.250, P < 0.001 for ALI; rho = 0.146, P < 0.001 for VI; rho = 0.271, P < 0.001 for PNI).
Conclusion: Subdivision of T3 colorectal cancer correlates with nodal and metastasis staging. Moreover, it correlates with other prognostic factors for colorectal cancer.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
