{"title":"低钾血症:常见病-回顾性调查。","authors":"Alasdair Reid, Gareth Jones, Chris Isles","doi":"10.1258/shorts.2012.011179","DOIUrl":null,"url":null,"abstract":"Objectives To define the causes of hypokalaemia in an unselected adult population. Design Retrospective survey of biochemistry database. Setting District general hospital in southwest Scotland. Participants and main outcome measures There were 187,704 measurements of urea and electrolytes in 2010. Sixty-one patients had serum potassium <2.5 mmol/L on at least one occasion. Results Average age of the patients was 71 (range 33–99) years. The most common causes were diarrhoea and/or vomiting (51% of cases), diuretic therapy (47%), nutritional causes including poor dietary intake, re-feeding syndrome and inadequate potassium supplementation when patients were nil by mouth (37%). In 25% of patients a transient and profound fall in serum potassium appeared to coincide with their acute illness. Acute alcohol intoxication and/or alcohol withdrawal were prominent features in 11% of patients. More than one cause was commonly present. There were no cases of Bartter's, Gitelman's or Liddle's syndromes or of hypokalaemic periodic paralysis in this study. Conclusions Severe hypokalaemia <2.5 mmol/L occurs at least once a week in a district general hospital with a catchment population of around 150,000, suggesting there may be around 300 cases a week in the UK (population around 50,000,000). Diuretics, vomiting and diarrhoea are commonly implicated as are nutritional causes, acute illness and alcohol. Bartter's, Gitelman's, Liddle's syndrome and hypokalaemic period paralysis are all extremely uncommon.","PeriodicalId":89182,"journal":{"name":"JRSM short reports","volume":"3 11","pages":"80"},"PeriodicalIF":0.0000,"publicationDate":"2012-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1258/shorts.2012.011179","citationCount":"17","resultStr":"{\"title\":\"Hypokalaemia: common things occur commonly - a retrospective survey.\",\"authors\":\"Alasdair Reid, Gareth Jones, Chris Isles\",\"doi\":\"10.1258/shorts.2012.011179\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Objectives To define the causes of hypokalaemia in an unselected adult population. Design Retrospective survey of biochemistry database. Setting District general hospital in southwest Scotland. Participants and main outcome measures There were 187,704 measurements of urea and electrolytes in 2010. Sixty-one patients had serum potassium <2.5 mmol/L on at least one occasion. Results Average age of the patients was 71 (range 33–99) years. The most common causes were diarrhoea and/or vomiting (51% of cases), diuretic therapy (47%), nutritional causes including poor dietary intake, re-feeding syndrome and inadequate potassium supplementation when patients were nil by mouth (37%). In 25% of patients a transient and profound fall in serum potassium appeared to coincide with their acute illness. Acute alcohol intoxication and/or alcohol withdrawal were prominent features in 11% of patients. More than one cause was commonly present. There were no cases of Bartter's, Gitelman's or Liddle's syndromes or of hypokalaemic periodic paralysis in this study. Conclusions Severe hypokalaemia <2.5 mmol/L occurs at least once a week in a district general hospital with a catchment population of around 150,000, suggesting there may be around 300 cases a week in the UK (population around 50,000,000). Diuretics, vomiting and diarrhoea are commonly implicated as are nutritional causes, acute illness and alcohol. Bartter's, Gitelman's, Liddle's syndrome and hypokalaemic period paralysis are all extremely uncommon.\",\"PeriodicalId\":89182,\"journal\":{\"name\":\"JRSM short reports\",\"volume\":\"3 11\",\"pages\":\"80\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2012-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1258/shorts.2012.011179\",\"citationCount\":\"17\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JRSM short reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1258/shorts.2012.011179\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2012/11/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JRSM short reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1258/shorts.2012.011179","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2012/11/30 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Hypokalaemia: common things occur commonly - a retrospective survey.
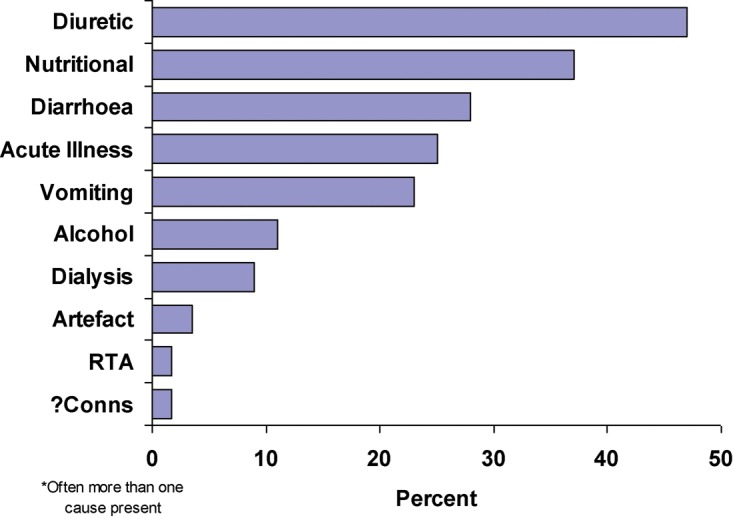
Objectives To define the causes of hypokalaemia in an unselected adult population. Design Retrospective survey of biochemistry database. Setting District general hospital in southwest Scotland. Participants and main outcome measures There were 187,704 measurements of urea and electrolytes in 2010. Sixty-one patients had serum potassium <2.5 mmol/L on at least one occasion. Results Average age of the patients was 71 (range 33–99) years. The most common causes were diarrhoea and/or vomiting (51% of cases), diuretic therapy (47%), nutritional causes including poor dietary intake, re-feeding syndrome and inadequate potassium supplementation when patients were nil by mouth (37%). In 25% of patients a transient and profound fall in serum potassium appeared to coincide with their acute illness. Acute alcohol intoxication and/or alcohol withdrawal were prominent features in 11% of patients. More than one cause was commonly present. There were no cases of Bartter's, Gitelman's or Liddle's syndromes or of hypokalaemic periodic paralysis in this study. Conclusions Severe hypokalaemia <2.5 mmol/L occurs at least once a week in a district general hospital with a catchment population of around 150,000, suggesting there may be around 300 cases a week in the UK (population around 50,000,000). Diuretics, vomiting and diarrhoea are commonly implicated as are nutritional causes, acute illness and alcohol. Bartter's, Gitelman's, Liddle's syndrome and hypokalaemic period paralysis are all extremely uncommon.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
