{"title":"242例肢端肥大症促生长激素垂体腺瘤的临床病理特征:根据激素分泌和细胞角蛋白分布进行分类。","authors":"Ryosuke Mori, Naoko Inoshita, Junko Takahashi-Fujigasaki, Tatsuhiro Joki, Hiroshi Nishioka, Toshiaki Abe, Takeshi Fujii, Shozo Yamada","doi":"10.1155/2013/723432","DOIUrl":null,"url":null,"abstract":"<p><p>The aim of this study was to clarify the relationship between the histological features of GH-producing adenomas surgically resected at the Toranomon Hospital and the clinical features of the patients. Histological examinations, including immunohistochemistry for anterior pituitary hormones and cytokeratin (CK), were performed on 242 consecutively excised GH-producing pituitary adenomas. Immunohistochemistry showed 45% of the adenomas to be monohormonal and 55% to be plurihormonal, producing GH-PRL (77%), GH-TSH (13%), and GH-PRL-TSH (10%). One-fourth of the monohormonal GH adenomas had a dot-like pattern of CK immunoreactivity in the majority of the tumor cells (>80%); they were significantly more common in female or younger patients and usually tended to be larger and more invasive than monohormonal GH adenomas with perinuclear CK. Interestingly, CK-immunonegative adenomas were found in only 5% of the patients; they also showed a tendency to be larger, suggesting that they are a distinct type of GH adenoma with clinically aggressive features. Serum hormone levels correlated well with tumor size only in GH-producing adenomas with a perinuclear pattern of CK immunoreactivity. Each histological subtype of adenoma, classified according to the pattern of CK immunoreactivity, was associated with distinct clinical characteristics. This information is useful for understanding the pathophysiology of acromegaly-causing GH-producing adenomas.</p>","PeriodicalId":89576,"journal":{"name":"ISRN endocrinology","volume":"2013 ","pages":"723432"},"PeriodicalIF":0.0000,"publicationDate":"2013-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2013/723432","citationCount":"35","resultStr":"{\"title\":\"Clinicopathological Features of Growth Hormone-Producing Pituitary Adenomas in 242 Acromegaly Patients: Classification according to Hormone Production and Cytokeratin Distribution.\",\"authors\":\"Ryosuke Mori, Naoko Inoshita, Junko Takahashi-Fujigasaki, Tatsuhiro Joki, Hiroshi Nishioka, Toshiaki Abe, Takeshi Fujii, Shozo Yamada\",\"doi\":\"10.1155/2013/723432\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The aim of this study was to clarify the relationship between the histological features of GH-producing adenomas surgically resected at the Toranomon Hospital and the clinical features of the patients. Histological examinations, including immunohistochemistry for anterior pituitary hormones and cytokeratin (CK), were performed on 242 consecutively excised GH-producing pituitary adenomas. Immunohistochemistry showed 45% of the adenomas to be monohormonal and 55% to be plurihormonal, producing GH-PRL (77%), GH-TSH (13%), and GH-PRL-TSH (10%). One-fourth of the monohormonal GH adenomas had a dot-like pattern of CK immunoreactivity in the majority of the tumor cells (>80%); they were significantly more common in female or younger patients and usually tended to be larger and more invasive than monohormonal GH adenomas with perinuclear CK. Interestingly, CK-immunonegative adenomas were found in only 5% of the patients; they also showed a tendency to be larger, suggesting that they are a distinct type of GH adenoma with clinically aggressive features. Serum hormone levels correlated well with tumor size only in GH-producing adenomas with a perinuclear pattern of CK immunoreactivity. Each histological subtype of adenoma, classified according to the pattern of CK immunoreactivity, was associated with distinct clinical characteristics. This information is useful for understanding the pathophysiology of acromegaly-causing GH-producing adenomas.</p>\",\"PeriodicalId\":89576,\"journal\":{\"name\":\"ISRN endocrinology\",\"volume\":\"2013 \",\"pages\":\"723432\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2013-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2013/723432\",\"citationCount\":\"35\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ISRN endocrinology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2013/723432\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2013/1/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ISRN endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2013/723432","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/1/21 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Clinicopathological Features of Growth Hormone-Producing Pituitary Adenomas in 242 Acromegaly Patients: Classification according to Hormone Production and Cytokeratin Distribution.
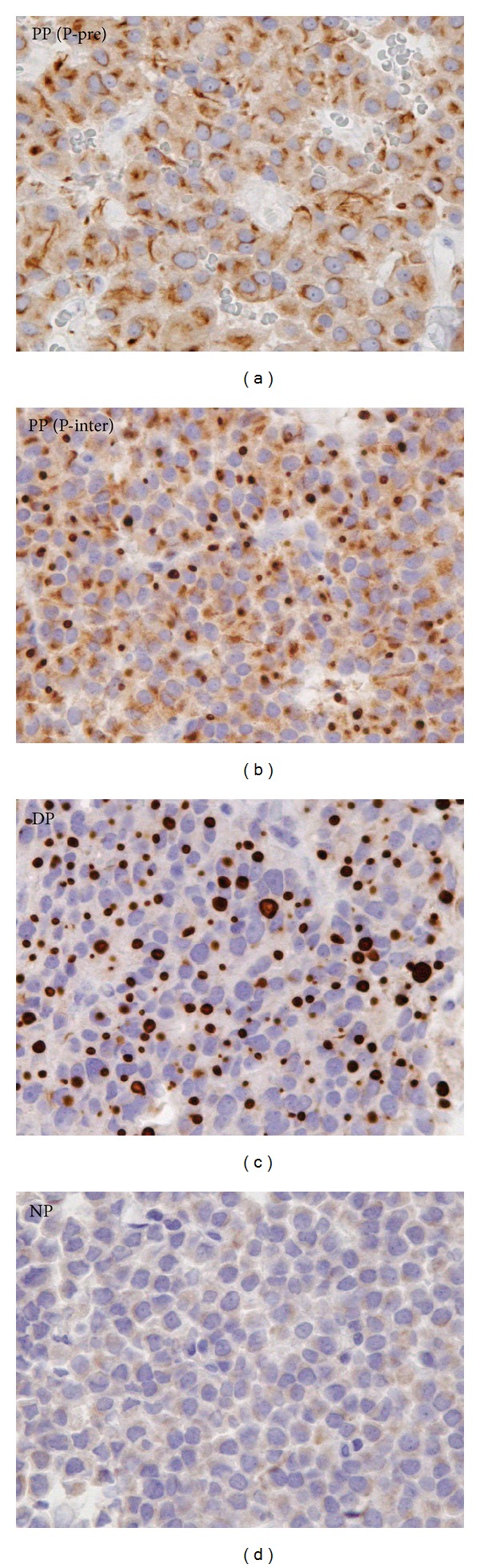
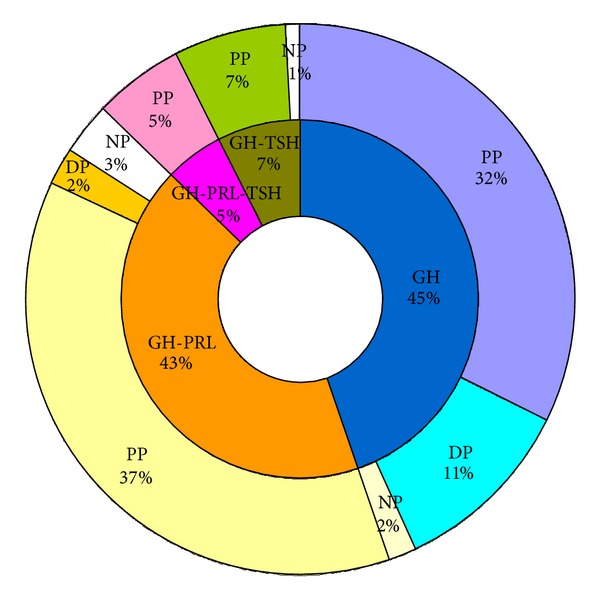
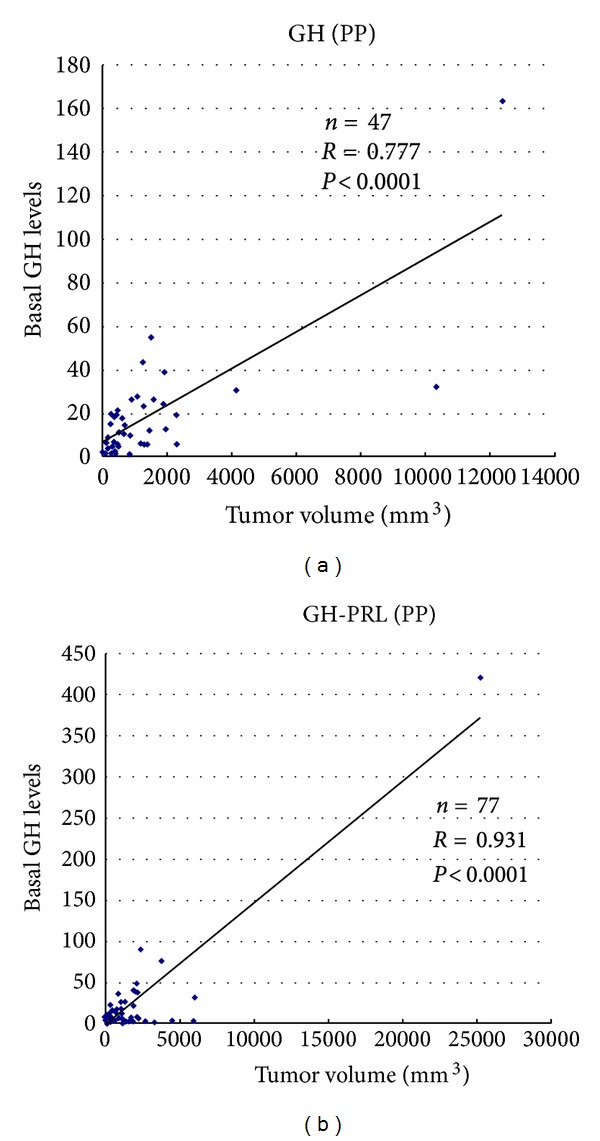
The aim of this study was to clarify the relationship between the histological features of GH-producing adenomas surgically resected at the Toranomon Hospital and the clinical features of the patients. Histological examinations, including immunohistochemistry for anterior pituitary hormones and cytokeratin (CK), were performed on 242 consecutively excised GH-producing pituitary adenomas. Immunohistochemistry showed 45% of the adenomas to be monohormonal and 55% to be plurihormonal, producing GH-PRL (77%), GH-TSH (13%), and GH-PRL-TSH (10%). One-fourth of the monohormonal GH adenomas had a dot-like pattern of CK immunoreactivity in the majority of the tumor cells (>80%); they were significantly more common in female or younger patients and usually tended to be larger and more invasive than monohormonal GH adenomas with perinuclear CK. Interestingly, CK-immunonegative adenomas were found in only 5% of the patients; they also showed a tendency to be larger, suggesting that they are a distinct type of GH adenoma with clinically aggressive features. Serum hormone levels correlated well with tumor size only in GH-producing adenomas with a perinuclear pattern of CK immunoreactivity. Each histological subtype of adenoma, classified according to the pattern of CK immunoreactivity, was associated with distinct clinical characteristics. This information is useful for understanding the pathophysiology of acromegaly-causing GH-producing adenomas.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
