{"title":"肾小球滤过率变化作为慢性肾脏疾病进展预测因素的有效性","authors":"Kunimi Maeda, Chieko Hamada, Satoshi Horikoshi, Yasuhiko Tomino","doi":"10.5402/2013/351364","DOIUrl":null,"url":null,"abstract":"<p><p>Purpose. To explore factors contributing to chronic kidney disease (CKD) progression and change in estimated glomerular filtration rate over time (ΔeGFR) as a risk factor in predialysis patients under multidisciplinary managements. Methods. Among 113 CKD patients, eGFR, serum creatinine, total protein, albumin, urea nitrogen, uric acid, calcium, inorganic phosphate, total cholesterol, urinary creatinine, urinary protein (UP), hemoglobin A1c, hemoglobin, and hematocrit were analyzed. Results. ΔeGFR analysis in the first six months presented a positive slope (remission group) in 43 patients (38%) and a negative slope (no-remission group) in 70 patients (62%). Three-year dialysis-free rate was 89.4% in the remission group and 39.3% in the no-remission group, with a significant difference (P < 0.0001). To explore factors contributing to dialysis initiation by stepwise Cox regression, baseline eGFR (HR 0.706, P < 0.0001) and ΔeGFR in the first six months of treatment (HR 0.075, P < 0.0001) were identified. To investigate factors affecting remission and no remission by stepwise logistic regression, age (odds ratio 1.06, P = 0.018) and UP excretion (odds ratio 1.223, P = 0.045) were identified. Conclusion. Monitoring of ΔeGFR and UP is not only useful in suppressing CKD 3 progression, but also in deciding strategies to achieve remission in individual patients. </p>","PeriodicalId":90192,"journal":{"name":"ISRN nephrology","volume":"2013 ","pages":"351364"},"PeriodicalIF":0.0000,"publicationDate":"2012-11-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4045413/pdf/","citationCount":"1","resultStr":"{\"title\":\"Usefulness of change in estimated glomerular filtration rate as a predicting factor of progression of chronic kidney disease.\",\"authors\":\"Kunimi Maeda, Chieko Hamada, Satoshi Horikoshi, Yasuhiko Tomino\",\"doi\":\"10.5402/2013/351364\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Purpose. To explore factors contributing to chronic kidney disease (CKD) progression and change in estimated glomerular filtration rate over time (ΔeGFR) as a risk factor in predialysis patients under multidisciplinary managements. Methods. Among 113 CKD patients, eGFR, serum creatinine, total protein, albumin, urea nitrogen, uric acid, calcium, inorganic phosphate, total cholesterol, urinary creatinine, urinary protein (UP), hemoglobin A1c, hemoglobin, and hematocrit were analyzed. Results. ΔeGFR analysis in the first six months presented a positive slope (remission group) in 43 patients (38%) and a negative slope (no-remission group) in 70 patients (62%). Three-year dialysis-free rate was 89.4% in the remission group and 39.3% in the no-remission group, with a significant difference (P < 0.0001). To explore factors contributing to dialysis initiation by stepwise Cox regression, baseline eGFR (HR 0.706, P < 0.0001) and ΔeGFR in the first six months of treatment (HR 0.075, P < 0.0001) were identified. To investigate factors affecting remission and no remission by stepwise logistic regression, age (odds ratio 1.06, P = 0.018) and UP excretion (odds ratio 1.223, P = 0.045) were identified. Conclusion. Monitoring of ΔeGFR and UP is not only useful in suppressing CKD 3 progression, but also in deciding strategies to achieve remission in individual patients. </p>\",\"PeriodicalId\":90192,\"journal\":{\"name\":\"ISRN nephrology\",\"volume\":\"2013 \",\"pages\":\"351364\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2012-11-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4045413/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"ISRN nephrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5402/2013/351364\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2013/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"ISRN nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5402/2013/351364","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2013/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
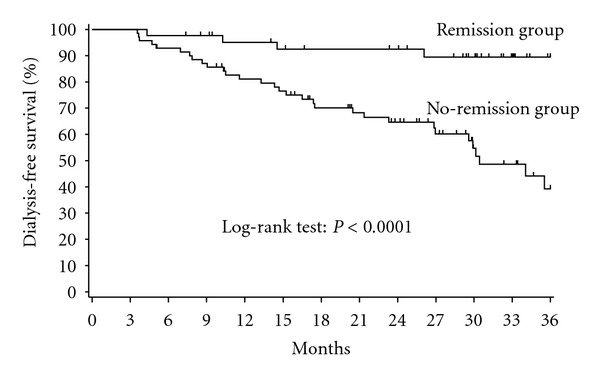
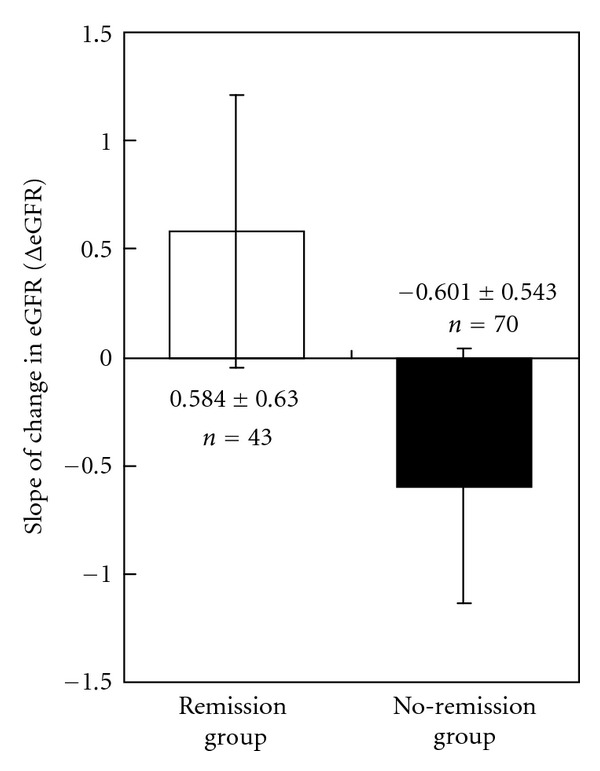
目的。在多学科管理下,探讨影响慢性肾脏疾病(CKD)进展的因素,以及估计肾小球滤过率随时间的变化(ΔeGFR)作为透析前患者的危险因素。方法。分析113例CKD患者的eGFR、血清肌酐、总蛋白、白蛋白、尿素氮、尿酸、钙、无机磷酸盐、总胆固醇、尿肌酐、尿蛋白(UP)、血红蛋白A1c、血红蛋白、红细胞压积。结果。ΔeGFR在前六个月的分析中,43名患者(38%)出现正斜率(缓解组),70名患者(62%)出现负斜率(无缓解组)。缓解组3年无透析率为89.4%,无缓解组为39.3%,差异有统计学意义(P < 0.0001)。为了通过逐步Cox回归探讨导致透析开始的因素,我们确定了治疗前6个月的基线eGFR (HR 0.706, P < 0.0001)和ΔeGFR (HR 0.075, P < 0.0001)。为探讨影响缓解和不缓解的因素,采用逐步logistic回归,确定年龄(优势比1.06,P = 0.018)和UP排泄(优势比1.223,P = 0.045)。结论。监测ΔeGFR和UP不仅对抑制CKD 3的进展有用,而且对决定个体患者实现缓解的策略也有用。
Usefulness of change in estimated glomerular filtration rate as a predicting factor of progression of chronic kidney disease.
Purpose. To explore factors contributing to chronic kidney disease (CKD) progression and change in estimated glomerular filtration rate over time (ΔeGFR) as a risk factor in predialysis patients under multidisciplinary managements. Methods. Among 113 CKD patients, eGFR, serum creatinine, total protein, albumin, urea nitrogen, uric acid, calcium, inorganic phosphate, total cholesterol, urinary creatinine, urinary protein (UP), hemoglobin A1c, hemoglobin, and hematocrit were analyzed. Results. ΔeGFR analysis in the first six months presented a positive slope (remission group) in 43 patients (38%) and a negative slope (no-remission group) in 70 patients (62%). Three-year dialysis-free rate was 89.4% in the remission group and 39.3% in the no-remission group, with a significant difference (P < 0.0001). To explore factors contributing to dialysis initiation by stepwise Cox regression, baseline eGFR (HR 0.706, P < 0.0001) and ΔeGFR in the first six months of treatment (HR 0.075, P < 0.0001) were identified. To investigate factors affecting remission and no remission by stepwise logistic regression, age (odds ratio 1.06, P = 0.018) and UP excretion (odds ratio 1.223, P = 0.045) were identified. Conclusion. Monitoring of ΔeGFR and UP is not only useful in suppressing CKD 3 progression, but also in deciding strategies to achieve remission in individual patients.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
