Raheleh Assari, Vahid Ziaee, Nima Parvaneh, Mohammad-Hassan Moradinejad
{"title":"周期性发热与中性粒细胞性皮肤病:是斯威特综合征吗?","authors":"Raheleh Assari, Vahid Ziaee, Nima Parvaneh, Mohammad-Hassan Moradinejad","doi":"10.1155/2014/320920","DOIUrl":null,"url":null,"abstract":"<p><p>A 7-year-old boy with high grade fever (39°C) and warm, erythematous, and indurated plaque above the left knee was referred. According to the previous records of this patient, these indurated plaques had been changed toward abscesses formation and then spontaneous drainage had occurred after about 6 to 7 days, and finally these lesions healed with scars. In multiple previous admissions, high grade fever, leukocytosis, and a noticeable increase in erythrocyte sedimentation rate and C-reactive protein were noted. After that, until 7th year of age, he had shoulder, gluteal, splenic, kidney, and left thigh lesions and pneumonia. The methylprednisolone pulse (30 mg/kg) was initiated with the diagnosis of Sweet's syndrome. After about 10-14 days, almost all of the laboratory data regressed to nearly normal limits. After about 5 months, he was admitted again with tachypnea and high grade fever and leukocytosis. After infusion of one methylprednisolone pulse, the fever and tachypnea resolved rapidly in about 24 hours. In this admission, colchicine (1 mg/kg) was added to the oral prednisolone after discharge. In the periodic fever and neutrophilic dermatosis, the rheumatologist should search for sterile abscesses in other organs. </p>","PeriodicalId":42865,"journal":{"name":"Case Reports in Immunology","volume":"2014 ","pages":"320920"},"PeriodicalIF":1.5000,"publicationDate":"2014-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2014/320920","citationCount":"3","resultStr":"{\"title\":\"Periodic Fever and Neutrophilic Dermatosis: Is It Sweet's Syndrome?\",\"authors\":\"Raheleh Assari, Vahid Ziaee, Nima Parvaneh, Mohammad-Hassan Moradinejad\",\"doi\":\"10.1155/2014/320920\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A 7-year-old boy with high grade fever (39°C) and warm, erythematous, and indurated plaque above the left knee was referred. According to the previous records of this patient, these indurated plaques had been changed toward abscesses formation and then spontaneous drainage had occurred after about 6 to 7 days, and finally these lesions healed with scars. In multiple previous admissions, high grade fever, leukocytosis, and a noticeable increase in erythrocyte sedimentation rate and C-reactive protein were noted. After that, until 7th year of age, he had shoulder, gluteal, splenic, kidney, and left thigh lesions and pneumonia. The methylprednisolone pulse (30 mg/kg) was initiated with the diagnosis of Sweet's syndrome. After about 10-14 days, almost all of the laboratory data regressed to nearly normal limits. After about 5 months, he was admitted again with tachypnea and high grade fever and leukocytosis. After infusion of one methylprednisolone pulse, the fever and tachypnea resolved rapidly in about 24 hours. In this admission, colchicine (1 mg/kg) was added to the oral prednisolone after discharge. In the periodic fever and neutrophilic dermatosis, the rheumatologist should search for sterile abscesses in other organs. </p>\",\"PeriodicalId\":42865,\"journal\":{\"name\":\"Case Reports in Immunology\",\"volume\":\"2014 \",\"pages\":\"320920\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2014-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2014/320920\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Immunology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2014/320920\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2014/12/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Immunology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2014/320920","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/12/4 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Periodic Fever and Neutrophilic Dermatosis: Is It Sweet's Syndrome?
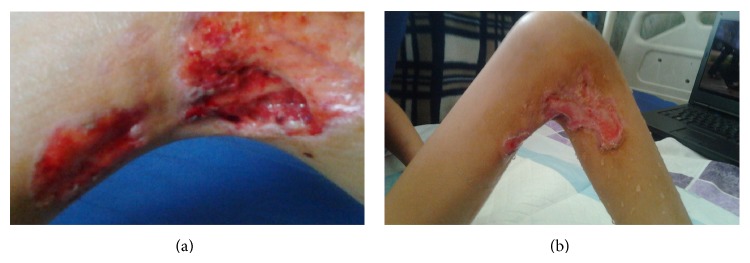
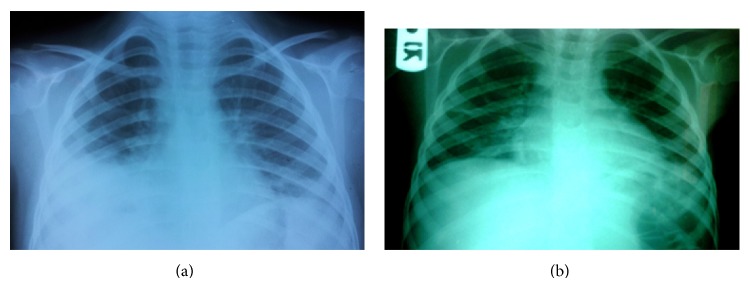
A 7-year-old boy with high grade fever (39°C) and warm, erythematous, and indurated plaque above the left knee was referred. According to the previous records of this patient, these indurated plaques had been changed toward abscesses formation and then spontaneous drainage had occurred after about 6 to 7 days, and finally these lesions healed with scars. In multiple previous admissions, high grade fever, leukocytosis, and a noticeable increase in erythrocyte sedimentation rate and C-reactive protein were noted. After that, until 7th year of age, he had shoulder, gluteal, splenic, kidney, and left thigh lesions and pneumonia. The methylprednisolone pulse (30 mg/kg) was initiated with the diagnosis of Sweet's syndrome. After about 10-14 days, almost all of the laboratory data regressed to nearly normal limits. After about 5 months, he was admitted again with tachypnea and high grade fever and leukocytosis. After infusion of one methylprednisolone pulse, the fever and tachypnea resolved rapidly in about 24 hours. In this admission, colchicine (1 mg/kg) was added to the oral prednisolone after discharge. In the periodic fever and neutrophilic dermatosis, the rheumatologist should search for sterile abscesses in other organs.
期刊介绍:
Case Reports in Immunology is a peer-reviewed, Open Access journal that publishes case reports and case series related to allergies, immunodeficiencies, autoimmune diseases, immune disorders, cancer immunology and transplantation immunology.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
