Lampros Kousoulas, Florian W R Vondran, Paulina Syryca, Juergen Klempnauer, Harald Schrem, Frank Lehner
{"title":"两次以上肾移植患者相关结果驱动因素的风险调整分析。","authors":"Lampros Kousoulas, Florian W R Vondran, Paulina Syryca, Juergen Klempnauer, Harald Schrem, Frank Lehner","doi":"10.1155/2015/712049","DOIUrl":null,"url":null,"abstract":"<p><p>Renal transplantation is the treatment of choice for patients suffering end-stage renal disease, but as the long-term renal allograft survival is limited, most transplant recipients will face graft loss and will be considered for a retransplantation. The goal of this study was to evaluate the patient and graft survival of the 61 renal transplant recipients after second or subsequent renal transplantation, transplanted in our institution between 1990 and 2010, and to identify risk factors related to inferior outcomes. Actuarial patient survival was 98.3%, 94.8%, and 88.2% after one, three, and five years, respectively. Actuarial graft survival was 86.8%, 80%, and 78.1% after one, three, and five years, respectively. Risk-adjusted analysis revealed that only age at the time of last transplantation had a significant influence on patient survival, whereas graft survival was influenced by multiple immunological and surgical factors, such as the number of HLA mismatches, the type of immunosuppression, the number of surgical complications, need of reoperation, primary graft nonfunction, and acute rejection episodes. In conclusion, third and subsequent renal transplantation constitute a valid therapeutic option, but inferior outcomes should be expected among elderly patients, hyperimmunized recipients, and recipients with multiple operations at the site of last renal transplantation. </p>","PeriodicalId":45795,"journal":{"name":"Journal of Transplantation","volume":"2015 ","pages":"712049"},"PeriodicalIF":2.2000,"publicationDate":"2015-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2015/712049","citationCount":"17","resultStr":"{\"title\":\"Risk-adjusted analysis of relevant outcome drivers for patients after more than two kidney transplants.\",\"authors\":\"Lampros Kousoulas, Florian W R Vondran, Paulina Syryca, Juergen Klempnauer, Harald Schrem, Frank Lehner\",\"doi\":\"10.1155/2015/712049\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Renal transplantation is the treatment of choice for patients suffering end-stage renal disease, but as the long-term renal allograft survival is limited, most transplant recipients will face graft loss and will be considered for a retransplantation. The goal of this study was to evaluate the patient and graft survival of the 61 renal transplant recipients after second or subsequent renal transplantation, transplanted in our institution between 1990 and 2010, and to identify risk factors related to inferior outcomes. Actuarial patient survival was 98.3%, 94.8%, and 88.2% after one, three, and five years, respectively. Actuarial graft survival was 86.8%, 80%, and 78.1% after one, three, and five years, respectively. Risk-adjusted analysis revealed that only age at the time of last transplantation had a significant influence on patient survival, whereas graft survival was influenced by multiple immunological and surgical factors, such as the number of HLA mismatches, the type of immunosuppression, the number of surgical complications, need of reoperation, primary graft nonfunction, and acute rejection episodes. In conclusion, third and subsequent renal transplantation constitute a valid therapeutic option, but inferior outcomes should be expected among elderly patients, hyperimmunized recipients, and recipients with multiple operations at the site of last renal transplantation. </p>\",\"PeriodicalId\":45795,\"journal\":{\"name\":\"Journal of Transplantation\",\"volume\":\"2015 \",\"pages\":\"712049\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2015-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2015/712049\",\"citationCount\":\"17\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Transplantation\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2015/712049\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2015/2/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2015/712049","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/2/1 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Risk-adjusted analysis of relevant outcome drivers for patients after more than two kidney transplants.
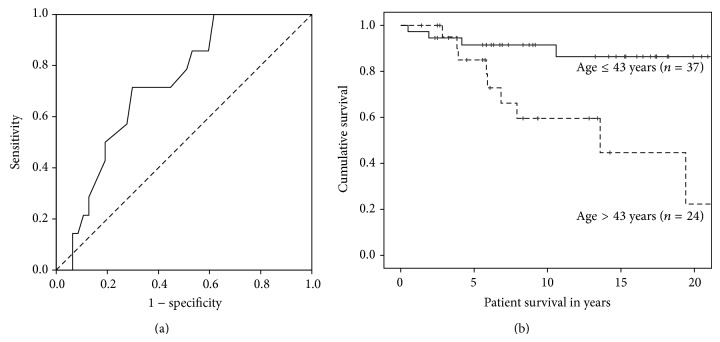
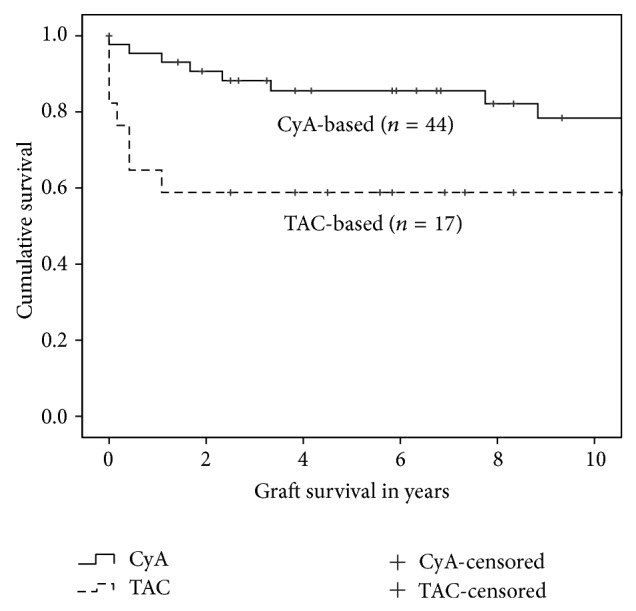
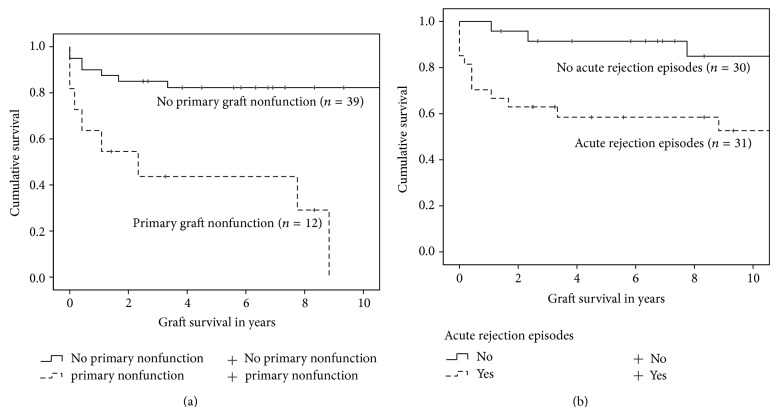
Renal transplantation is the treatment of choice for patients suffering end-stage renal disease, but as the long-term renal allograft survival is limited, most transplant recipients will face graft loss and will be considered for a retransplantation. The goal of this study was to evaluate the patient and graft survival of the 61 renal transplant recipients after second or subsequent renal transplantation, transplanted in our institution between 1990 and 2010, and to identify risk factors related to inferior outcomes. Actuarial patient survival was 98.3%, 94.8%, and 88.2% after one, three, and five years, respectively. Actuarial graft survival was 86.8%, 80%, and 78.1% after one, three, and five years, respectively. Risk-adjusted analysis revealed that only age at the time of last transplantation had a significant influence on patient survival, whereas graft survival was influenced by multiple immunological and surgical factors, such as the number of HLA mismatches, the type of immunosuppression, the number of surgical complications, need of reoperation, primary graft nonfunction, and acute rejection episodes. In conclusion, third and subsequent renal transplantation constitute a valid therapeutic option, but inferior outcomes should be expected among elderly patients, hyperimmunized recipients, and recipients with multiple operations at the site of last renal transplantation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
