Rick B. Delamarter MD , Daniel Murrey MD , Michael E. Janssen DO , Jeffrey A. Goldstein MD , Jack Zigler MD , Bobby K.-B. Tay MD , Bruce Darden II MD
{"title":"结果来自前瞻性、随机、多中心研究器械豁免试验ProDisc-C与前路颈椎椎间盘切除术和融合的对比,随访4年,持续访问患者24个月","authors":"Rick B. Delamarter MD , Daniel Murrey MD , Michael E. Janssen DO , Jeffrey A. Goldstein MD , Jack Zigler MD , Bobby K.-B. Tay MD , Bruce Darden II MD","doi":"10.1016/j.esas.2010.09.001","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Cervical total disk replacement (TDR) is intended to address pain and preserve motion between vertebral bodies in patients with symptomatic cervical disk disease. Two-year follow-up for the ProDisc-C (Synthes USA Products, LLC, West Chester, Pennsylvania) TDR clinical trial showed non-inferiority versus anterior cervical discectomy and fusion (ACDF), showing superiority in many clinical outcomes. We present the 4-year interim follow-up results.</p></div><div><h3>Methods</h3><p>Patients were randomized (1:1) to ProDisc-C (PDC-R) or ACDF. Patients were assessed preoperatively, and postoperatively at 6 weeks and 3, 6, 12, 18, 24, 36, and 48 months. After the randomized portion, continued access (CA) patients also underwent ProDisc-C implantation, with follow-up visits up to 24 months. Evaluations included Neck Disability Index (NDI), Visual Analog Scale (VAS) for pain/satisfaction, and radiographic and physical/neurologic examinations.</p></div><div><h3>Results</h3><p>Randomized patients (103 PDC-R and 106 ACDF) and 136 CA patients were treated at 13 sites. VAS pain and NDI score improvements from baseline were significant for all patients (<em>P</em> < .0001) but did not differ among groups. VAS satisfaction was higher at all time points for PDC-R versus ACDF patients (<em>P</em> = .0499 at 48 months). The percentage of patients who responded yes to surgery again was 85.6% at 24 months and 88.9% at 48 months in the PDC-R group, 80.9% at 24 months and 81.0% at 48 months in the ACDF group, and 86.3% at 24 months in the CA group. Five PDC-R patients (48 months) and no CA patients (24 months) had index-level bridging bone. By 48 months, approximately 4-fold more ACDF patients required secondary surgery (3 of 103 PDC-R patients [2.9%] vs 12 of 106 ACDF patients [11.3%], <em>P</em> = .0292). Of these, 6 ACDF patients (5.6%) required procedures at adjacent levels. Three CA patients required secondary procedures (24 months).</p></div><div><h3>Conclusions</h3><p>Our 4-year data support that ProDisc-C TDR and ACDF are viable surgical options for symptomatic cervical disk disease. Although ACDF patients may be at higher risk for additional surgical intervention, patients in both groups show good clinical results at longer-term follow-up.</p></div>","PeriodicalId":88695,"journal":{"name":"SAS journal","volume":"4 4","pages":"Pages 122-128"},"PeriodicalIF":0.0000,"publicationDate":"2010-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.esas.2010.09.001","citationCount":"97","resultStr":"{\"title\":\"Results at 24 months from the prospective, randomized, multicenter Investigational Device Exemption trial of ProDisc-C versus anterior cervical discectomy and fusion with 4-year follow-up and continued access patients\",\"authors\":\"Rick B. Delamarter MD , Daniel Murrey MD , Michael E. Janssen DO , Jeffrey A. Goldstein MD , Jack Zigler MD , Bobby K.-B. Tay MD , Bruce Darden II MD\",\"doi\":\"10.1016/j.esas.2010.09.001\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Cervical total disk replacement (TDR) is intended to address pain and preserve motion between vertebral bodies in patients with symptomatic cervical disk disease. Two-year follow-up for the ProDisc-C (Synthes USA Products, LLC, West Chester, Pennsylvania) TDR clinical trial showed non-inferiority versus anterior cervical discectomy and fusion (ACDF), showing superiority in many clinical outcomes. We present the 4-year interim follow-up results.</p></div><div><h3>Methods</h3><p>Patients were randomized (1:1) to ProDisc-C (PDC-R) or ACDF. Patients were assessed preoperatively, and postoperatively at 6 weeks and 3, 6, 12, 18, 24, 36, and 48 months. After the randomized portion, continued access (CA) patients also underwent ProDisc-C implantation, with follow-up visits up to 24 months. Evaluations included Neck Disability Index (NDI), Visual Analog Scale (VAS) for pain/satisfaction, and radiographic and physical/neurologic examinations.</p></div><div><h3>Results</h3><p>Randomized patients (103 PDC-R and 106 ACDF) and 136 CA patients were treated at 13 sites. VAS pain and NDI score improvements from baseline were significant for all patients (<em>P</em> < .0001) but did not differ among groups. VAS satisfaction was higher at all time points for PDC-R versus ACDF patients (<em>P</em> = .0499 at 48 months). The percentage of patients who responded yes to surgery again was 85.6% at 24 months and 88.9% at 48 months in the PDC-R group, 80.9% at 24 months and 81.0% at 48 months in the ACDF group, and 86.3% at 24 months in the CA group. Five PDC-R patients (48 months) and no CA patients (24 months) had index-level bridging bone. By 48 months, approximately 4-fold more ACDF patients required secondary surgery (3 of 103 PDC-R patients [2.9%] vs 12 of 106 ACDF patients [11.3%], <em>P</em> = .0292). Of these, 6 ACDF patients (5.6%) required procedures at adjacent levels. Three CA patients required secondary procedures (24 months).</p></div><div><h3>Conclusions</h3><p>Our 4-year data support that ProDisc-C TDR and ACDF are viable surgical options for symptomatic cervical disk disease. Although ACDF patients may be at higher risk for additional surgical intervention, patients in both groups show good clinical results at longer-term follow-up.</p></div>\",\"PeriodicalId\":88695,\"journal\":{\"name\":\"SAS journal\",\"volume\":\"4 4\",\"pages\":\"Pages 122-128\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2010-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1016/j.esas.2010.09.001\",\"citationCount\":\"97\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"SAS journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1935981010000769\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2010/9/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAS journal","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1935981010000769","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2010/9/29 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 97
摘要
背景颈椎全椎间盘置换术(TDR)旨在解决症状性颈椎间盘疾病患者的疼痛并保持椎体之间的运动。对ProDisc-C (Synthes USA Products, LLC, West Chester, Pennsylvania) TDR临床试验的两年随访显示,与前路颈椎椎间盘切除术和融合(ACDF)相比,非劣效性,在许多临床结果上显示出优势。我们报告了4年的中期随访结果。方法将患者按1:1的比例随机分配到ProDisc-C (PDC-R)或ACDF组。术前和术后分别于6周、3、6、12、18、24、36和48个月对患者进行评估。在随机部分之后,继续访问(CA)患者也接受了ProDisc-C植入,随访长达24个月。评估包括颈部残疾指数(NDI)、疼痛/满意度视觉模拟量表(VAS)、放射学和物理/神经学检查。结果随机分组患者(103例PDC-R和106例ACDF)和136例CA患者在13个部位接受治疗。所有患者的VAS疼痛和NDI评分较基线均有显著改善(P <.0001),但组间无差异。与ACDF患者相比,PDC-R患者在所有时间点的VAS满意度更高(48个月时P = 0.0499)。pd - r组再次手术的患者比例分别为:24个月时85.6%和48个月时88.9%,ACDF组24个月时80.9%和48个月时81.0%,CA组24个月时86.3%。5例PDC-R患者(48个月)和无CA患者(24个月)有指数水平桥接骨。到48个月时,大约4倍的ACDF患者需要二次手术(103例pd - r患者中有3例[2.9%],106例ACDF患者中有12例[11.3%],P = 0.0292)。其中,6例ACDF患者(5.6%)需要在邻近水平进行手术。3例CA患者需要二次手术(24个月)。结论4年数据支持ProDisc-C TDR和ACDF是治疗症状性颈椎间盘病的可行手术选择。虽然ACDF患者可能有更高的风险进行额外的手术干预,但两组患者在长期随访中均表现出良好的临床结果。
Results at 24 months from the prospective, randomized, multicenter Investigational Device Exemption trial of ProDisc-C versus anterior cervical discectomy and fusion with 4-year follow-up and continued access patients
Background
Cervical total disk replacement (TDR) is intended to address pain and preserve motion between vertebral bodies in patients with symptomatic cervical disk disease. Two-year follow-up for the ProDisc-C (Synthes USA Products, LLC, West Chester, Pennsylvania) TDR clinical trial showed non-inferiority versus anterior cervical discectomy and fusion (ACDF), showing superiority in many clinical outcomes. We present the 4-year interim follow-up results.
Methods
Patients were randomized (1:1) to ProDisc-C (PDC-R) or ACDF. Patients were assessed preoperatively, and postoperatively at 6 weeks and 3, 6, 12, 18, 24, 36, and 48 months. After the randomized portion, continued access (CA) patients also underwent ProDisc-C implantation, with follow-up visits up to 24 months. Evaluations included Neck Disability Index (NDI), Visual Analog Scale (VAS) for pain/satisfaction, and radiographic and physical/neurologic examinations.
Results
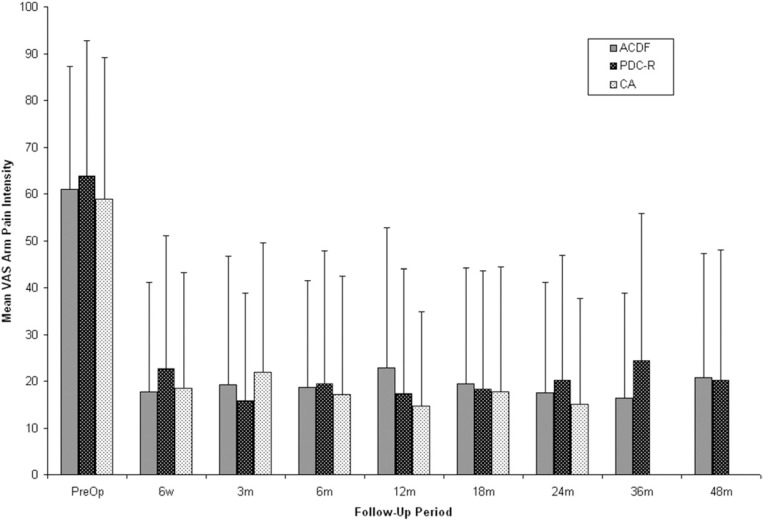
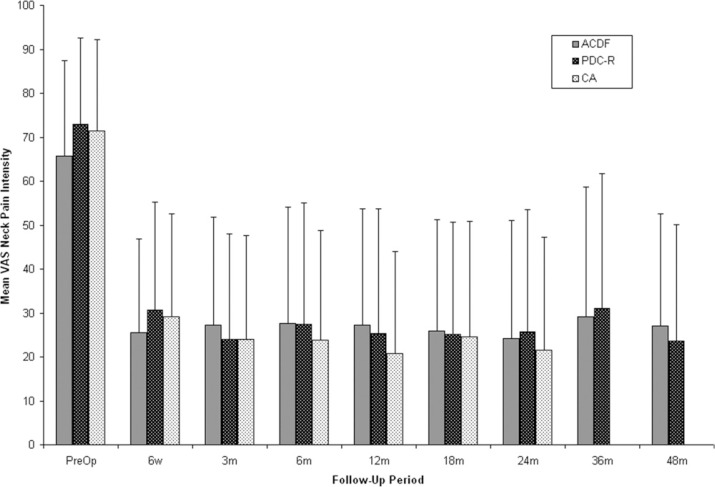
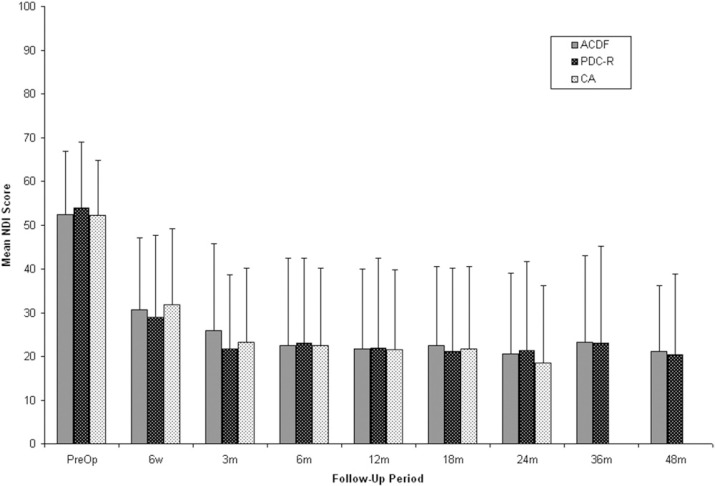
Randomized patients (103 PDC-R and 106 ACDF) and 136 CA patients were treated at 13 sites. VAS pain and NDI score improvements from baseline were significant for all patients (P < .0001) but did not differ among groups. VAS satisfaction was higher at all time points for PDC-R versus ACDF patients (P = .0499 at 48 months). The percentage of patients who responded yes to surgery again was 85.6% at 24 months and 88.9% at 48 months in the PDC-R group, 80.9% at 24 months and 81.0% at 48 months in the ACDF group, and 86.3% at 24 months in the CA group. Five PDC-R patients (48 months) and no CA patients (24 months) had index-level bridging bone. By 48 months, approximately 4-fold more ACDF patients required secondary surgery (3 of 103 PDC-R patients [2.9%] vs 12 of 106 ACDF patients [11.3%], P = .0292). Of these, 6 ACDF patients (5.6%) required procedures at adjacent levels. Three CA patients required secondary procedures (24 months).
Conclusions
Our 4-year data support that ProDisc-C TDR and ACDF are viable surgical options for symptomatic cervical disk disease. Although ACDF patients may be at higher risk for additional surgical intervention, patients in both groups show good clinical results at longer-term follow-up.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
