M G Zeier, Imani Masimango, Nathalie Demoulin, Alice Leroy, Samir Saadi, Laura Labriola
{"title":"血液透析病人不寻常的皮肤损伤。","authors":"M G Zeier, Imani Masimango, Nathalie Demoulin, Alice Leroy, Samir Saadi, Laura Labriola","doi":"10.1093/ndtplus/sfr120","DOIUrl":null,"url":null,"abstract":"A 71-year-old woman of Turkish origin presented in July 2009 to our haemodialysis unit with multiple painless, non-pruritic, reddish-purple skin lesions on legs and feet. She had been on peritoneal dialysis from July 2006 to December 2008 for presumed diabetic nephropathy and then shifted to haemodialysis due to recurrent peritonitis. She was under low-dose steroids since February 2008 for seropositive polyarthritis. Steroids were increased in May 2009 following a third sub-occlusive episode due to sclerosing encapsulating peritonitis. At presentation, she was taking methylprednisolone (12 mg per day), aspirin, omeprazole, atorvastatin, gabapentin, clonazepam, calcium carbonate and insulin. Clinical examination showed multiple infracentimetric dark red to violaceous non-tender macules, papules and nodules on legs and feet (Figure 1). No ulceration or necrosis was visible. No inguinal lymph nodes were palpable. Physical examination revealed no other new finding.","PeriodicalId":18987,"journal":{"name":"NDT Plus","volume":"4 6","pages":"443-4"},"PeriodicalIF":0.0000,"publicationDate":"2011-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1093/ndtplus/sfr120","citationCount":"0","resultStr":"{\"title\":\"Unusual skin lesions in a haemodialyzed patient.\",\"authors\":\"M G Zeier, Imani Masimango, Nathalie Demoulin, Alice Leroy, Samir Saadi, Laura Labriola\",\"doi\":\"10.1093/ndtplus/sfr120\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"A 71-year-old woman of Turkish origin presented in July 2009 to our haemodialysis unit with multiple painless, non-pruritic, reddish-purple skin lesions on legs and feet. She had been on peritoneal dialysis from July 2006 to December 2008 for presumed diabetic nephropathy and then shifted to haemodialysis due to recurrent peritonitis. She was under low-dose steroids since February 2008 for seropositive polyarthritis. Steroids were increased in May 2009 following a third sub-occlusive episode due to sclerosing encapsulating peritonitis. At presentation, she was taking methylprednisolone (12 mg per day), aspirin, omeprazole, atorvastatin, gabapentin, clonazepam, calcium carbonate and insulin. Clinical examination showed multiple infracentimetric dark red to violaceous non-tender macules, papules and nodules on legs and feet (Figure 1). No ulceration or necrosis was visible. No inguinal lymph nodes were palpable. Physical examination revealed no other new finding.\",\"PeriodicalId\":18987,\"journal\":{\"name\":\"NDT Plus\",\"volume\":\"4 6\",\"pages\":\"443-4\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2011-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1093/ndtplus/sfr120\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NDT Plus\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ndtplus/sfr120\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NDT Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ndtplus/sfr120","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
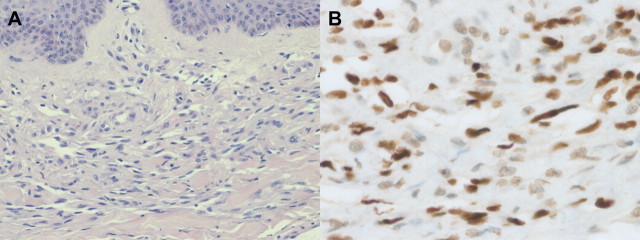
A 71-year-old woman of Turkish origin presented in July 2009 to our haemodialysis unit with multiple painless, non-pruritic, reddish-purple skin lesions on legs and feet. She had been on peritoneal dialysis from July 2006 to December 2008 for presumed diabetic nephropathy and then shifted to haemodialysis due to recurrent peritonitis. She was under low-dose steroids since February 2008 for seropositive polyarthritis. Steroids were increased in May 2009 following a third sub-occlusive episode due to sclerosing encapsulating peritonitis. At presentation, she was taking methylprednisolone (12 mg per day), aspirin, omeprazole, atorvastatin, gabapentin, clonazepam, calcium carbonate and insulin. Clinical examination showed multiple infracentimetric dark red to violaceous non-tender macules, papules and nodules on legs and feet (Figure 1). No ulceration or necrosis was visible. No inguinal lymph nodes were palpable. Physical examination revealed no other new finding.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
