{"title":"内窥镜辅助零位第一肋骨切除术治疗胸廓出口综合征的中期结果。","authors":"Hiroshi Satake, Ryusuke Honma, Toshiya Nito, Yasushi Naganuma, Junichiro Shibuya, Masahiro Maruyama, Tomohiro Uno, Michiaki Takagi","doi":"10.1093/icvts/ivac239","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>We have hypothesized that an endoscopically assisted transaxillary approach in the zero position would be able to improve visualization and allow safe surgery for thoracic outlet syndrome.</p><p><strong>Methods: </strong>We performed surgery only for patients with certain objective findings, including blood flow disruption, low blood flow and accelerated blood flow in the subclavian artery demonstrated using Doppler sonography, narrowing of the scalene interval width between the anterior and middle interscalene muscles (interscalene base) or costoclavicular space demonstrated using Duplex ultrasonography or computed tomography angiography. The present study included 45 consecutive patients (50 limbs) who underwent endoscopic transaxillary first rib resection with scalenotomy and brachial plexus neurolysis. We assessed the intraoperative parameters, including the interscalene base, blood loss, operation time, patient satisfaction, preoperative and postoperative Quick Disability of the Arm, Shoulder and Hand and complications.</p><p><strong>Results: </strong>The mean intraoperatively measured interscalene base width was 6.4 mm. All patients showed improvement after surgery. The outcome was excellent in 40% of cases, good in 48%, fair in 12% and poor in none. Pneumothorax was present in 6%. There were no other complications and no recurrences. Among patients who had been followed up for at least 2 years, the Quick Disability of the Arm, Shoulder and Hand score was significantly improved (42 before surgery vs 12 at final follow-up), especially in athletes relative to non-athletes (0.2 vs 16). The present approach achieved complete relief in 43% of cases overall (91% in athletes and 16% in non-athletes).</p><p><strong>Conclusions: </strong>Endoscopically assisted transaxillary first rib resection and brachial plexus neurolysis in the zero position are useful and safe for thoracic outlet syndrome, especially in athletes.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-09-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a4/e1/ivac239.PMC9536291.pdf","citationCount":"0","resultStr":"{\"title\":\"Midterm results of endoscopically assisted first rib resection in the zero position for thoracic outlet syndrome.\",\"authors\":\"Hiroshi Satake, Ryusuke Honma, Toshiya Nito, Yasushi Naganuma, Junichiro Shibuya, Masahiro Maruyama, Tomohiro Uno, Michiaki Takagi\",\"doi\":\"10.1093/icvts/ivac239\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>We have hypothesized that an endoscopically assisted transaxillary approach in the zero position would be able to improve visualization and allow safe surgery for thoracic outlet syndrome.</p><p><strong>Methods: </strong>We performed surgery only for patients with certain objective findings, including blood flow disruption, low blood flow and accelerated blood flow in the subclavian artery demonstrated using Doppler sonography, narrowing of the scalene interval width between the anterior and middle interscalene muscles (interscalene base) or costoclavicular space demonstrated using Duplex ultrasonography or computed tomography angiography. The present study included 45 consecutive patients (50 limbs) who underwent endoscopic transaxillary first rib resection with scalenotomy and brachial plexus neurolysis. We assessed the intraoperative parameters, including the interscalene base, blood loss, operation time, patient satisfaction, preoperative and postoperative Quick Disability of the Arm, Shoulder and Hand and complications.</p><p><strong>Results: </strong>The mean intraoperatively measured interscalene base width was 6.4 mm. All patients showed improvement after surgery. The outcome was excellent in 40% of cases, good in 48%, fair in 12% and poor in none. Pneumothorax was present in 6%. There were no other complications and no recurrences. Among patients who had been followed up for at least 2 years, the Quick Disability of the Arm, Shoulder and Hand score was significantly improved (42 before surgery vs 12 at final follow-up), especially in athletes relative to non-athletes (0.2 vs 16). The present approach achieved complete relief in 43% of cases overall (91% in athletes and 16% in non-athletes).</p><p><strong>Conclusions: </strong>Endoscopically assisted transaxillary first rib resection and brachial plexus neurolysis in the zero position are useful and safe for thoracic outlet syndrome, especially in athletes.</p>\",\"PeriodicalId\":13621,\"journal\":{\"name\":\"Interactive cardiovascular and thoracic surgery\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2022-09-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a4/e1/ivac239.PMC9536291.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Interactive cardiovascular and thoracic surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/icvts/ivac239\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac239","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Midterm results of endoscopically assisted first rib resection in the zero position for thoracic outlet syndrome.
Objectives: We have hypothesized that an endoscopically assisted transaxillary approach in the zero position would be able to improve visualization and allow safe surgery for thoracic outlet syndrome.
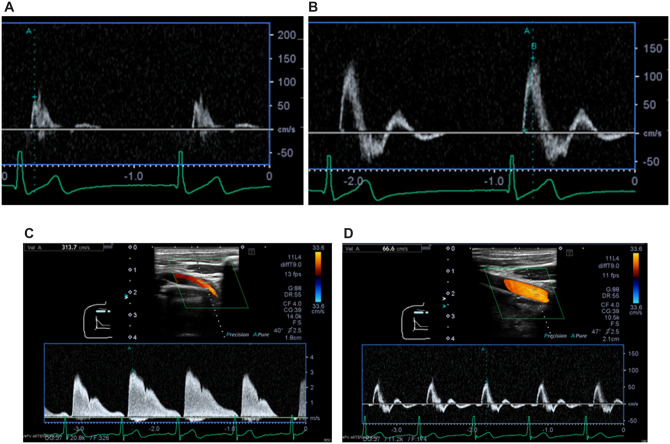
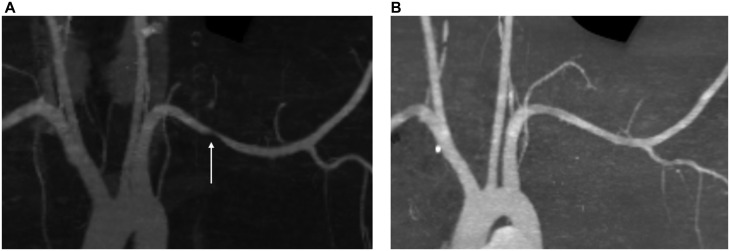
Methods: We performed surgery only for patients with certain objective findings, including blood flow disruption, low blood flow and accelerated blood flow in the subclavian artery demonstrated using Doppler sonography, narrowing of the scalene interval width between the anterior and middle interscalene muscles (interscalene base) or costoclavicular space demonstrated using Duplex ultrasonography or computed tomography angiography. The present study included 45 consecutive patients (50 limbs) who underwent endoscopic transaxillary first rib resection with scalenotomy and brachial plexus neurolysis. We assessed the intraoperative parameters, including the interscalene base, blood loss, operation time, patient satisfaction, preoperative and postoperative Quick Disability of the Arm, Shoulder and Hand and complications.
Results: The mean intraoperatively measured interscalene base width was 6.4 mm. All patients showed improvement after surgery. The outcome was excellent in 40% of cases, good in 48%, fair in 12% and poor in none. Pneumothorax was present in 6%. There were no other complications and no recurrences. Among patients who had been followed up for at least 2 years, the Quick Disability of the Arm, Shoulder and Hand score was significantly improved (42 before surgery vs 12 at final follow-up), especially in athletes relative to non-athletes (0.2 vs 16). The present approach achieved complete relief in 43% of cases overall (91% in athletes and 16% in non-athletes).
Conclusions: Endoscopically assisted transaxillary first rib resection and brachial plexus neurolysis in the zero position are useful and safe for thoracic outlet syndrome, especially in athletes.
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
