Riccardo Guanà, Andrea Carpino, Giuseppe Garbagni, Cecilia Morchio, Salvatore Garofalo, Alessandro Pane, Federico Scottoni, Elisa Zambaiti, Giulia Perucca, Elena Madonia, Fabrizio Gennari
{"title":"内窥镜治疗11岁女童电池插入后严重阴道狭窄。","authors":"Riccardo Guanà, Andrea Carpino, Giuseppe Garbagni, Cecilia Morchio, Salvatore Garofalo, Alessandro Pane, Federico Scottoni, Elisa Zambaiti, Giulia Perucca, Elena Madonia, Fabrizio Gennari","doi":"10.1055/a-1920-5849","DOIUrl":null,"url":null,"abstract":"<p><p>Acquired vaginal strictures are rare entities in children. As a result, they are generally difficult to manage and tend to recur despite appropriate initial therapy. This case study reports the staged management of vaginal stenosis following the insertion of a button battery. In this case, an 11-year-old girl experienced at 4 years old a battery insertion in the vaginal canal by her neighbor's son, who was 6-year-old at the time. Two weeks from insertion, the parents noted the foreign body discharge spontaneously. The girl had not complained of any symptoms at the time and had been asymptomatic for many years. In November 2020, she came to the emergency department reporting cramping abdominal pain accompanied by mucopurulent discharge. An abdominal ultrasound showed the presence of hematometrocolpos, and a vaginal stenosis dilation under general anesthesia was performed the following day. After 3 weeks, the stenosis was still present, preventing the passage of Hegar number 4. The girl was subjected to a vaginoscopic stenosis resection utilizing a monopolar hook passed through an operative channel. A Bakri catheter filled with 120 mL of water was left in place. After 10 days, the girl was discharged home with the Bakri inserted. Two weeks after discharge, she was reevaluated in the outpatient setting, where the Bakri was removed with no signs of residual stenosis. Acquired vaginal stenosis could be demanding to treat, particularly with the sole conservative approach. A first-line option can be the Hegar dilation. The endoscopic approach can be a second-line, minimally invasive treatment, but long-term outcomes are difficult to predict.</p>","PeriodicalId":43204,"journal":{"name":"European Journal of Pediatric Surgery Reports","volume":" ","pages":"e135-e140"},"PeriodicalIF":0.7000,"publicationDate":"2022-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9484869/pdf/","citationCount":"1","resultStr":"{\"title\":\"Endoscopic Treatment of a Severe Vaginal Stenosis Following Battery Insertion in an 11-Year-Old Girl.\",\"authors\":\"Riccardo Guanà, Andrea Carpino, Giuseppe Garbagni, Cecilia Morchio, Salvatore Garofalo, Alessandro Pane, Federico Scottoni, Elisa Zambaiti, Giulia Perucca, Elena Madonia, Fabrizio Gennari\",\"doi\":\"10.1055/a-1920-5849\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Acquired vaginal strictures are rare entities in children. As a result, they are generally difficult to manage and tend to recur despite appropriate initial therapy. This case study reports the staged management of vaginal stenosis following the insertion of a button battery. In this case, an 11-year-old girl experienced at 4 years old a battery insertion in the vaginal canal by her neighbor's son, who was 6-year-old at the time. Two weeks from insertion, the parents noted the foreign body discharge spontaneously. The girl had not complained of any symptoms at the time and had been asymptomatic for many years. In November 2020, she came to the emergency department reporting cramping abdominal pain accompanied by mucopurulent discharge. An abdominal ultrasound showed the presence of hematometrocolpos, and a vaginal stenosis dilation under general anesthesia was performed the following day. After 3 weeks, the stenosis was still present, preventing the passage of Hegar number 4. The girl was subjected to a vaginoscopic stenosis resection utilizing a monopolar hook passed through an operative channel. A Bakri catheter filled with 120 mL of water was left in place. After 10 days, the girl was discharged home with the Bakri inserted. Two weeks after discharge, she was reevaluated in the outpatient setting, where the Bakri was removed with no signs of residual stenosis. Acquired vaginal stenosis could be demanding to treat, particularly with the sole conservative approach. A first-line option can be the Hegar dilation. The endoscopic approach can be a second-line, minimally invasive treatment, but long-term outcomes are difficult to predict.</p>\",\"PeriodicalId\":43204,\"journal\":{\"name\":\"European Journal of Pediatric Surgery Reports\",\"volume\":\" \",\"pages\":\"e135-e140\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2022-09-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9484869/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Pediatric Surgery Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-1920-5849\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pediatric Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-1920-5849","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Endoscopic Treatment of a Severe Vaginal Stenosis Following Battery Insertion in an 11-Year-Old Girl.
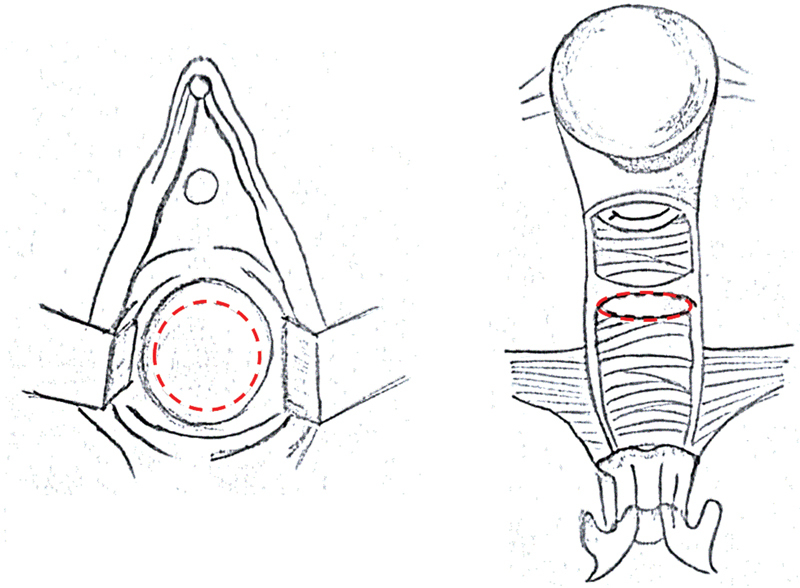
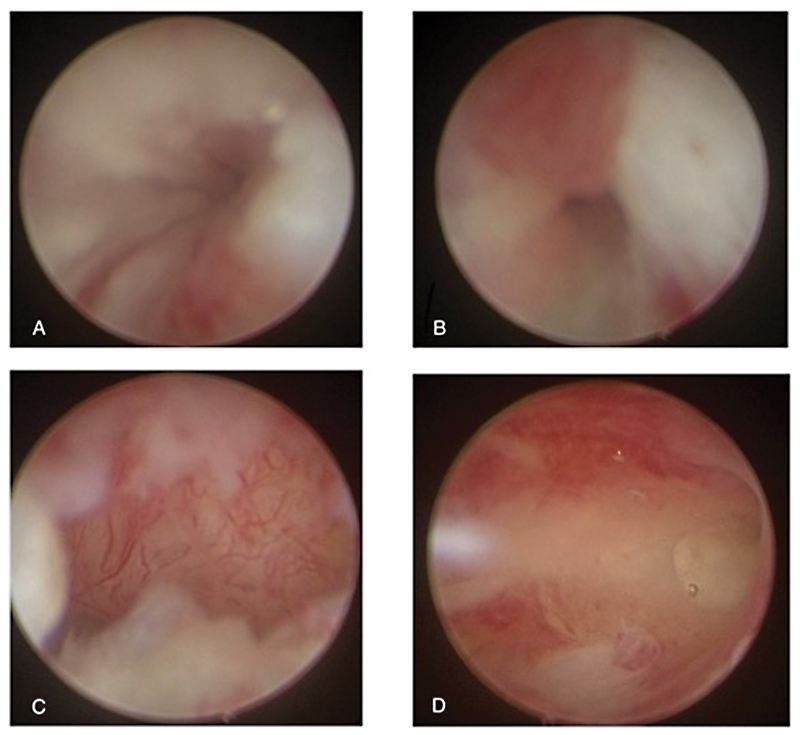
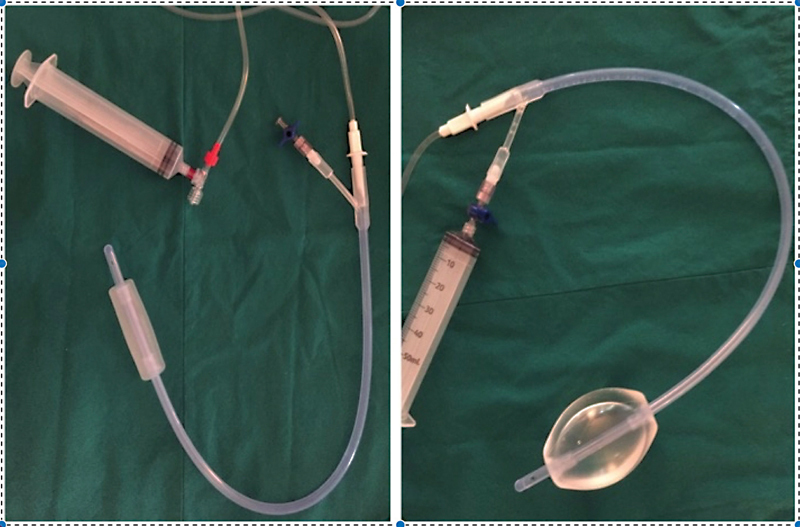
Acquired vaginal strictures are rare entities in children. As a result, they are generally difficult to manage and tend to recur despite appropriate initial therapy. This case study reports the staged management of vaginal stenosis following the insertion of a button battery. In this case, an 11-year-old girl experienced at 4 years old a battery insertion in the vaginal canal by her neighbor's son, who was 6-year-old at the time. Two weeks from insertion, the parents noted the foreign body discharge spontaneously. The girl had not complained of any symptoms at the time and had been asymptomatic for many years. In November 2020, she came to the emergency department reporting cramping abdominal pain accompanied by mucopurulent discharge. An abdominal ultrasound showed the presence of hematometrocolpos, and a vaginal stenosis dilation under general anesthesia was performed the following day. After 3 weeks, the stenosis was still present, preventing the passage of Hegar number 4. The girl was subjected to a vaginoscopic stenosis resection utilizing a monopolar hook passed through an operative channel. A Bakri catheter filled with 120 mL of water was left in place. After 10 days, the girl was discharged home with the Bakri inserted. Two weeks after discharge, she was reevaluated in the outpatient setting, where the Bakri was removed with no signs of residual stenosis. Acquired vaginal stenosis could be demanding to treat, particularly with the sole conservative approach. A first-line option can be the Hegar dilation. The endoscopic approach can be a second-line, minimally invasive treatment, but long-term outcomes are difficult to predict.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
