William Reiche, Abubakar Tauseef, Ahmed Sabri, Mohsin Mirza, David Cantu, Peter Silberstein, Saurabh Chandan
{"title":"移植后淋巴细胞增生性疾病患者的胃肠道表现、危险因素和治疗:一项系统综述。","authors":"William Reiche, Abubakar Tauseef, Ahmed Sabri, Mohsin Mirza, David Cantu, Peter Silberstein, Saurabh Chandan","doi":"10.5500/wjt.v12.i8.268","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with a history of solid organ transplantation (SOT) or hematopoietic stem cell transplantation (HSCT) are at an increased risk of developing post-transplant lymphoproliferative disorder (PTLD). The gastrointestinal (GI) tract is commonly affected as it has an abundance of B and T cells.</p><p><strong>Aim: </strong>To determine typical GI-manifestations, risk factors for developing PTLD, and management.</p><p><strong>Methods: </strong>Major databases were searched until November 2021.</p><p><strong>Results: </strong>Non-case report studies that described GI manifestations of PTLD, risk factors for developing PTLD, and management of PTLD were included. Nine articles written within the last 20 years were included in the review. All articles found that patients with a history of SOT, regardless of transplanted organ, have a propensity to develop GI-PTLD.</p><p><strong>Conclusion: </strong>GI tract manifestations may be nonspecific; therefore, consideration of risk factors is crucial for identifying GI-PTLD. Like other lymphoma variants, PTLD is very aggressive making early diagnosis key to prognosis. Initial treatment is reduction of immunosuppression which is effective in more than 50% of cases; however, additional therapy including rituximab, chemotherapy, and surgery may also be required.</p>","PeriodicalId":68893,"journal":{"name":"世界移植杂志(英文版)","volume":"12 8","pages":"268-280"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a4/d8/WJT-12-268.PMC9453293.pdf","citationCount":"2","resultStr":"{\"title\":\"Gastrointestinal manifestations, risk factors, and management in patients with post-transplant lymphoproliferative disorder: A systematic review.\",\"authors\":\"William Reiche, Abubakar Tauseef, Ahmed Sabri, Mohsin Mirza, David Cantu, Peter Silberstein, Saurabh Chandan\",\"doi\":\"10.5500/wjt.v12.i8.268\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients with a history of solid organ transplantation (SOT) or hematopoietic stem cell transplantation (HSCT) are at an increased risk of developing post-transplant lymphoproliferative disorder (PTLD). The gastrointestinal (GI) tract is commonly affected as it has an abundance of B and T cells.</p><p><strong>Aim: </strong>To determine typical GI-manifestations, risk factors for developing PTLD, and management.</p><p><strong>Methods: </strong>Major databases were searched until November 2021.</p><p><strong>Results: </strong>Non-case report studies that described GI manifestations of PTLD, risk factors for developing PTLD, and management of PTLD were included. Nine articles written within the last 20 years were included in the review. All articles found that patients with a history of SOT, regardless of transplanted organ, have a propensity to develop GI-PTLD.</p><p><strong>Conclusion: </strong>GI tract manifestations may be nonspecific; therefore, consideration of risk factors is crucial for identifying GI-PTLD. Like other lymphoma variants, PTLD is very aggressive making early diagnosis key to prognosis. Initial treatment is reduction of immunosuppression which is effective in more than 50% of cases; however, additional therapy including rituximab, chemotherapy, and surgery may also be required.</p>\",\"PeriodicalId\":68893,\"journal\":{\"name\":\"世界移植杂志(英文版)\",\"volume\":\"12 8\",\"pages\":\"268-280\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-08-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a4/d8/WJT-12-268.PMC9453293.pdf\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"世界移植杂志(英文版)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5500/wjt.v12.i8.268\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界移植杂志(英文版)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5500/wjt.v12.i8.268","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Gastrointestinal manifestations, risk factors, and management in patients with post-transplant lymphoproliferative disorder: A systematic review.
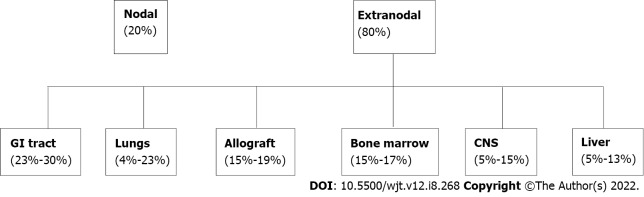
Background: Patients with a history of solid organ transplantation (SOT) or hematopoietic stem cell transplantation (HSCT) are at an increased risk of developing post-transplant lymphoproliferative disorder (PTLD). The gastrointestinal (GI) tract is commonly affected as it has an abundance of B and T cells.
Aim: To determine typical GI-manifestations, risk factors for developing PTLD, and management.
Methods: Major databases were searched until November 2021.
Results: Non-case report studies that described GI manifestations of PTLD, risk factors for developing PTLD, and management of PTLD were included. Nine articles written within the last 20 years were included in the review. All articles found that patients with a history of SOT, regardless of transplanted organ, have a propensity to develop GI-PTLD.
Conclusion: GI tract manifestations may be nonspecific; therefore, consideration of risk factors is crucial for identifying GI-PTLD. Like other lymphoma variants, PTLD is very aggressive making early diagnosis key to prognosis. Initial treatment is reduction of immunosuppression which is effective in more than 50% of cases; however, additional therapy including rituximab, chemotherapy, and surgery may also be required.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
