Sergey Nikolaevich Novikov, Roman Vladimirovich Novikov, Yurii Olegovich Merezhko, Mariya Yurevna Gotovchikova, Nikolai Dmitrievich Ilin, Yulia Sergeevna Melnik, Sergey Vasilevich Kanaev
{"title":"高、高危前列腺癌择期骨盆照射后高剂量率近距离放疗与立体定向放射治疗的比较。","authors":"Sergey Nikolaevich Novikov, Roman Vladimirovich Novikov, Yurii Olegovich Merezhko, Mariya Yurevna Gotovchikova, Nikolai Dmitrievich Ilin, Yulia Sergeevna Melnik, Sergey Vasilevich Kanaev","doi":"10.3857/roj.2022.00339","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To compare biochemical recurrence-free survival (BRFS) and toxicity outcomes of high dose rate brachytherapy (HDRB) and stereotactic body radiotherapy (SBRT) boost after elective nodal irradiation for high/very high-risk prostate cancer.</p><p><strong>Materials and methods: </strong>a retrospective analysis was performed in 149 male. In 98 patients, the boost to the prostate was delivered by HDRB as 2 fractions of 10 Gy (EQD2 for α/β = 1.5; 66 Gy) or 1 fraction of 15 Gy (EQD2 for α/β = 1.5; 71 Gy). In 51 male, SBRT was used for the boost delivery (3 fractions of 7 Gy; EQD2Gy for α/β = 1.5; 51 Gy) because brachytherapy equipment was out of order.</p><p><strong>Results: </strong>In 98 patients that received HDRB boost, 3- and 5-year BRFS were 74.6% and 66.8%. Late grade-II genitourinary toxicity was detected in 27, grade-III in 1 case. Grade-II (maximum) rectal toxicity was diagnosed in nine patients. For 51 male patients that received SBRT boost, 3- and 5-year BRFS was 76.5% and 67.7%. Late grade-II (maximum) genitourinary toxicity was detected in five cases, late grade-II rectal toxicity in four cases. Other three patients developed late grade-III-IV rectal toxicity that required diverting colostomy. SBRT boost was associated with higher maximum dose to 2 cm3 of anterior rectal wall (D2cm³rectum) compared to HDRB: 92% versus 55% of dose to prostate. Severe rectal toxicity was negligible at EQD2 D2cm³rectum <85 Gy and EQD2 D5cm³ rectum <75 Gy.</p><p><strong>Conclusion: </strong>Our results indicate similar 3- and 5-year BRFS in patients with high/very high-risk prostate cancer who received HDRB or SBRT boost, but SBRT boost is associated with higher rate of severe late rectal toxicity.</p>","PeriodicalId":46572,"journal":{"name":"Radiation Oncology Journal","volume":"40 3","pages":"200-207"},"PeriodicalIF":2.2000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/65/roj-2022-00339.PMC9535414.pdf","citationCount":"1","resultStr":"{\"title\":\"A comparison between high dose rate brachytherapy and stereotactic body radiotherapy boost after elective pelvic irradiation for high and very high-risk prostate cancer.\",\"authors\":\"Sergey Nikolaevich Novikov, Roman Vladimirovich Novikov, Yurii Olegovich Merezhko, Mariya Yurevna Gotovchikova, Nikolai Dmitrievich Ilin, Yulia Sergeevna Melnik, Sergey Vasilevich Kanaev\",\"doi\":\"10.3857/roj.2022.00339\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To compare biochemical recurrence-free survival (BRFS) and toxicity outcomes of high dose rate brachytherapy (HDRB) and stereotactic body radiotherapy (SBRT) boost after elective nodal irradiation for high/very high-risk prostate cancer.</p><p><strong>Materials and methods: </strong>a retrospective analysis was performed in 149 male. In 98 patients, the boost to the prostate was delivered by HDRB as 2 fractions of 10 Gy (EQD2 for α/β = 1.5; 66 Gy) or 1 fraction of 15 Gy (EQD2 for α/β = 1.5; 71 Gy). In 51 male, SBRT was used for the boost delivery (3 fractions of 7 Gy; EQD2Gy for α/β = 1.5; 51 Gy) because brachytherapy equipment was out of order.</p><p><strong>Results: </strong>In 98 patients that received HDRB boost, 3- and 5-year BRFS were 74.6% and 66.8%. Late grade-II genitourinary toxicity was detected in 27, grade-III in 1 case. Grade-II (maximum) rectal toxicity was diagnosed in nine patients. For 51 male patients that received SBRT boost, 3- and 5-year BRFS was 76.5% and 67.7%. Late grade-II (maximum) genitourinary toxicity was detected in five cases, late grade-II rectal toxicity in four cases. Other three patients developed late grade-III-IV rectal toxicity that required diverting colostomy. SBRT boost was associated with higher maximum dose to 2 cm3 of anterior rectal wall (D2cm³rectum) compared to HDRB: 92% versus 55% of dose to prostate. Severe rectal toxicity was negligible at EQD2 D2cm³rectum <85 Gy and EQD2 D5cm³ rectum <75 Gy.</p><p><strong>Conclusion: </strong>Our results indicate similar 3- and 5-year BRFS in patients with high/very high-risk prostate cancer who received HDRB or SBRT boost, but SBRT boost is associated with higher rate of severe late rectal toxicity.</p>\",\"PeriodicalId\":46572,\"journal\":{\"name\":\"Radiation Oncology Journal\",\"volume\":\"40 3\",\"pages\":\"200-207\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2022-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/65/roj-2022-00339.PMC9535414.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiation Oncology Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3857/roj.2022.00339\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/9/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2022.00339","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
A comparison between high dose rate brachytherapy and stereotactic body radiotherapy boost after elective pelvic irradiation for high and very high-risk prostate cancer.
Purpose: To compare biochemical recurrence-free survival (BRFS) and toxicity outcomes of high dose rate brachytherapy (HDRB) and stereotactic body radiotherapy (SBRT) boost after elective nodal irradiation for high/very high-risk prostate cancer.
Materials and methods: a retrospective analysis was performed in 149 male. In 98 patients, the boost to the prostate was delivered by HDRB as 2 fractions of 10 Gy (EQD2 for α/β = 1.5; 66 Gy) or 1 fraction of 15 Gy (EQD2 for α/β = 1.5; 71 Gy). In 51 male, SBRT was used for the boost delivery (3 fractions of 7 Gy; EQD2Gy for α/β = 1.5; 51 Gy) because brachytherapy equipment was out of order.
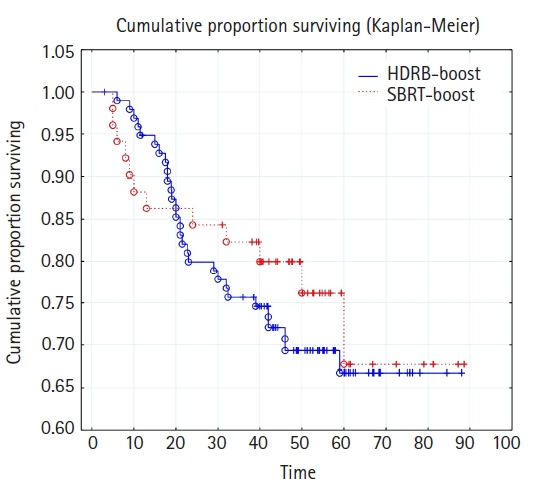
Results: In 98 patients that received HDRB boost, 3- and 5-year BRFS were 74.6% and 66.8%. Late grade-II genitourinary toxicity was detected in 27, grade-III in 1 case. Grade-II (maximum) rectal toxicity was diagnosed in nine patients. For 51 male patients that received SBRT boost, 3- and 5-year BRFS was 76.5% and 67.7%. Late grade-II (maximum) genitourinary toxicity was detected in five cases, late grade-II rectal toxicity in four cases. Other three patients developed late grade-III-IV rectal toxicity that required diverting colostomy. SBRT boost was associated with higher maximum dose to 2 cm3 of anterior rectal wall (D2cm³rectum) compared to HDRB: 92% versus 55% of dose to prostate. Severe rectal toxicity was negligible at EQD2 D2cm³rectum <85 Gy and EQD2 D5cm³ rectum <75 Gy.
Conclusion: Our results indicate similar 3- and 5-year BRFS in patients with high/very high-risk prostate cancer who received HDRB or SBRT boost, but SBRT boost is associated with higher rate of severe late rectal toxicity.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
