Harriet Rachel Kagoya, Dan Kibuule, Timothy William Rennie, Honoré Kabwebwe Mitonga
{"title":"在资源有限的情况下,加强高质量医药卫生系统数据效用的模型。","authors":"Harriet Rachel Kagoya, Dan Kibuule, Timothy William Rennie, Honoré Kabwebwe Mitonga","doi":"10.1177/2399202620940267","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Limited utility of quality health data undermines efforts to strengthen healthcare delivery, particularly in resource-limited settings. Few studies model the effective utility of quality pharmaceutical information system (PIS) data in sub-Saharan Africa, typified with weak health systems.</p><p><strong>Aim: </strong>To develop a model and guidelines for strengthening utility of quality PIS data in public healthcare in Namibia, a resource-limited setting.</p><p><strong>Methods: </strong>A qualitative model based on Dickoff et al. practice-oriented theory, Chinn and Jacobs' systematic approach to theory, and applied consensus techniques. Data from nationwide studies on quality and utility of PIS data in public healthcare conducted between 2018 and March 2020 informed the development of the model concepts. Pharmaceutical and public health systems experts validated the final model.</p><p><strong>Results: </strong>Overall, four preliminary national studies that recruited 58 PIS focal persons at 38 public health facilities and national level informed the development of four model concepts. The model describes concepts on access, management, dissemination, and utility of quality PIS data. Activities to implement the model in practice include grass-root integration of real-time automated pharmaceutical intelligence systems to collect, consolidate, monitor, and report PIS data. Strengthening coordination, human resources, and technical capacity through support supervisory systems at grass-root facilities are key activities. PIS focal persons at health facility and national level are agents to implement these activities among recipients, that is, healthcare professionals at points of care. Guidelines for implementation of the model at point of care are included. Experts described the model as clear, simple, comprehensive, and integration of pharmaceutical intelligence systems at point of care as novel and of importance to enhance utility of quality PIS data in resource-limited settings.</p><p><strong>Conclusion: </strong>While utility of quality PIS data is limited in Namibia, advantages of the model are encouraging, toward building resilient pharmaceutical intelligence systems at grass roots in resource-limited countries, where there are not only weak health systems, but high burden of misuse of medicines.</p>","PeriodicalId":74158,"journal":{"name":"Medicine access @ point of care","volume":"4 ","pages":"2399202620940267"},"PeriodicalIF":0.0000,"publicationDate":"2020-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2399202620940267","citationCount":"3","resultStr":"{\"title\":\"A model to strengthen utility of quality pharmaceutical health systems data in resource-limited settings.\",\"authors\":\"Harriet Rachel Kagoya, Dan Kibuule, Timothy William Rennie, Honoré Kabwebwe Mitonga\",\"doi\":\"10.1177/2399202620940267\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Limited utility of quality health data undermines efforts to strengthen healthcare delivery, particularly in resource-limited settings. Few studies model the effective utility of quality pharmaceutical information system (PIS) data in sub-Saharan Africa, typified with weak health systems.</p><p><strong>Aim: </strong>To develop a model and guidelines for strengthening utility of quality PIS data in public healthcare in Namibia, a resource-limited setting.</p><p><strong>Methods: </strong>A qualitative model based on Dickoff et al. practice-oriented theory, Chinn and Jacobs' systematic approach to theory, and applied consensus techniques. Data from nationwide studies on quality and utility of PIS data in public healthcare conducted between 2018 and March 2020 informed the development of the model concepts. Pharmaceutical and public health systems experts validated the final model.</p><p><strong>Results: </strong>Overall, four preliminary national studies that recruited 58 PIS focal persons at 38 public health facilities and national level informed the development of four model concepts. The model describes concepts on access, management, dissemination, and utility of quality PIS data. Activities to implement the model in practice include grass-root integration of real-time automated pharmaceutical intelligence systems to collect, consolidate, monitor, and report PIS data. Strengthening coordination, human resources, and technical capacity through support supervisory systems at grass-root facilities are key activities. PIS focal persons at health facility and national level are agents to implement these activities among recipients, that is, healthcare professionals at points of care. Guidelines for implementation of the model at point of care are included. Experts described the model as clear, simple, comprehensive, and integration of pharmaceutical intelligence systems at point of care as novel and of importance to enhance utility of quality PIS data in resource-limited settings.</p><p><strong>Conclusion: </strong>While utility of quality PIS data is limited in Namibia, advantages of the model are encouraging, toward building resilient pharmaceutical intelligence systems at grass roots in resource-limited countries, where there are not only weak health systems, but high burden of misuse of medicines.</p>\",\"PeriodicalId\":74158,\"journal\":{\"name\":\"Medicine access @ point of care\",\"volume\":\"4 \",\"pages\":\"2399202620940267\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-07-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/2399202620940267\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medicine access @ point of care\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/2399202620940267\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medicine access @ point of care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2399202620940267","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
A model to strengthen utility of quality pharmaceutical health systems data in resource-limited settings.
Background: Limited utility of quality health data undermines efforts to strengthen healthcare delivery, particularly in resource-limited settings. Few studies model the effective utility of quality pharmaceutical information system (PIS) data in sub-Saharan Africa, typified with weak health systems.
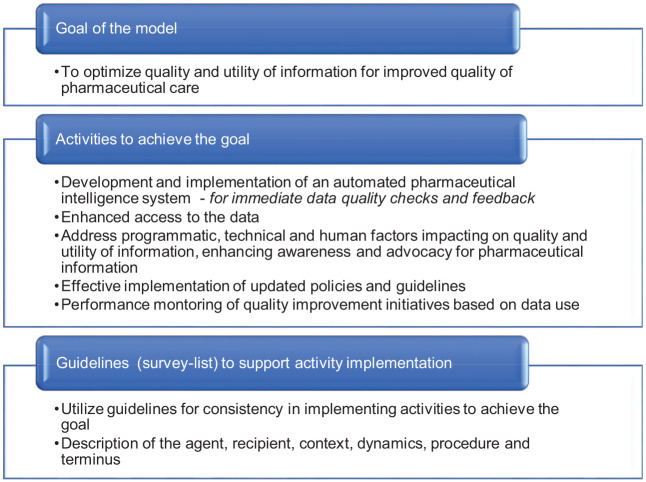
Aim: To develop a model and guidelines for strengthening utility of quality PIS data in public healthcare in Namibia, a resource-limited setting.
Methods: A qualitative model based on Dickoff et al. practice-oriented theory, Chinn and Jacobs' systematic approach to theory, and applied consensus techniques. Data from nationwide studies on quality and utility of PIS data in public healthcare conducted between 2018 and March 2020 informed the development of the model concepts. Pharmaceutical and public health systems experts validated the final model.
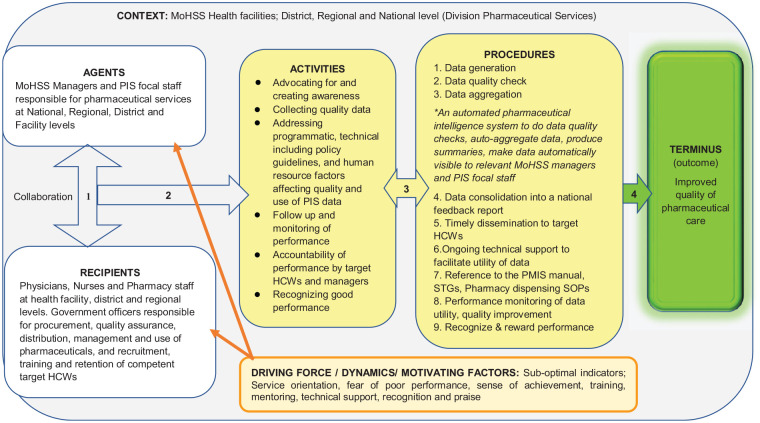
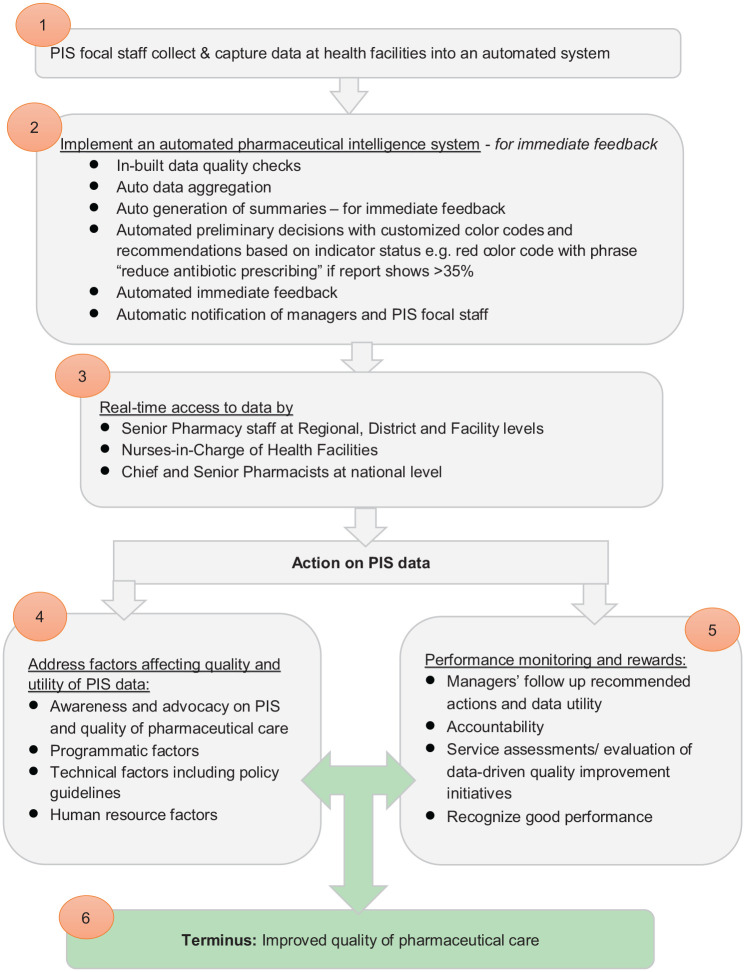
Results: Overall, four preliminary national studies that recruited 58 PIS focal persons at 38 public health facilities and national level informed the development of four model concepts. The model describes concepts on access, management, dissemination, and utility of quality PIS data. Activities to implement the model in practice include grass-root integration of real-time automated pharmaceutical intelligence systems to collect, consolidate, monitor, and report PIS data. Strengthening coordination, human resources, and technical capacity through support supervisory systems at grass-root facilities are key activities. PIS focal persons at health facility and national level are agents to implement these activities among recipients, that is, healthcare professionals at points of care. Guidelines for implementation of the model at point of care are included. Experts described the model as clear, simple, comprehensive, and integration of pharmaceutical intelligence systems at point of care as novel and of importance to enhance utility of quality PIS data in resource-limited settings.
Conclusion: While utility of quality PIS data is limited in Namibia, advantages of the model are encouraging, toward building resilient pharmaceutical intelligence systems at grass roots in resource-limited countries, where there are not only weak health systems, but high burden of misuse of medicines.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
