{"title":"根治性膀胱切除术前膀胱肿瘤经尿道完全切除不是器官限制性膀胱癌的危险因素:一项病例对照研究。","authors":"Xiaoxu Yuan, Mingkun Chen, Jing Yang, Yunlin Ye","doi":"10.1097/CU9.0000000000000110","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To investigate the role of complete transurethral resection of bladder tumor (TURBT) before radical cystectomy (RC) for organ-confined bladder cancer.</p><p><strong>Materials and methods: </strong>Data of patients who underwent RC in our center from January 2008 to December 2018 were retrospectively reviewed. Patients with >T2N0M0 disease and positive surgical margins and those who received neoadjuvant/adjuvant chemotherapy or radiotherapy were excluded. Complete TURBT was defined as no visible lesion under endoscopic examination after TURBT or in the bladder specimen after RC. Kaplan-Meier curves and log-rank tests assessed disease-free survival (DFS). Logistic and Cox regression analyses were performed to identify potential predictors.</p><p><strong>Results: </strong>A total of 236 patients were included in this review, including 207 males, with a median age of 61 years. The median tumor size was 3 cm, and a total of 94 patients had identified pathological T2 stage disease. Complete TURBT was correlated with tumor size (<i>p</i> = 0.041), histological variants (<i>p</i> = 0.026), and down-staging (<i>p</i> < 0.001). Tumor size, grade, and histological variants were independent predictors of complete TURBT. During a median follow-up of 42.7 months, 30 patients developed disease recurrence. Age and histological variants were independent predictors of DFS (<i>p</i> = 0.022 and 0.032, respectively), whereas complete TURBT was not an independent predictor of DFS (<i>p</i> = 0.156). Down-staging was not associated with survival outcome.</p><p><strong>Conclusions: </strong>Complete TURBT was correlated with an increased rate of down-staging before RC. It was not associated with better oncologic outcomes for patients with organ-confined bladder cancer.</p>","PeriodicalId":39147,"journal":{"name":"Current Urology","volume":"16 3","pages":"142-146"},"PeriodicalIF":0.9000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2c/16/curr-urol-16-142.PMC9527917.pdf","citationCount":"0","resultStr":"{\"title\":\"Complete transurethral resection of bladder tumor before radical cystectomy is not a risk factor for organ-confined bladder cancer: A case-control study.\",\"authors\":\"Xiaoxu Yuan, Mingkun Chen, Jing Yang, Yunlin Ye\",\"doi\":\"10.1097/CU9.0000000000000110\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To investigate the role of complete transurethral resection of bladder tumor (TURBT) before radical cystectomy (RC) for organ-confined bladder cancer.</p><p><strong>Materials and methods: </strong>Data of patients who underwent RC in our center from January 2008 to December 2018 were retrospectively reviewed. Patients with >T2N0M0 disease and positive surgical margins and those who received neoadjuvant/adjuvant chemotherapy or radiotherapy were excluded. Complete TURBT was defined as no visible lesion under endoscopic examination after TURBT or in the bladder specimen after RC. Kaplan-Meier curves and log-rank tests assessed disease-free survival (DFS). Logistic and Cox regression analyses were performed to identify potential predictors.</p><p><strong>Results: </strong>A total of 236 patients were included in this review, including 207 males, with a median age of 61 years. The median tumor size was 3 cm, and a total of 94 patients had identified pathological T2 stage disease. Complete TURBT was correlated with tumor size (<i>p</i> = 0.041), histological variants (<i>p</i> = 0.026), and down-staging (<i>p</i> < 0.001). Tumor size, grade, and histological variants were independent predictors of complete TURBT. During a median follow-up of 42.7 months, 30 patients developed disease recurrence. Age and histological variants were independent predictors of DFS (<i>p</i> = 0.022 and 0.032, respectively), whereas complete TURBT was not an independent predictor of DFS (<i>p</i> = 0.156). Down-staging was not associated with survival outcome.</p><p><strong>Conclusions: </strong>Complete TURBT was correlated with an increased rate of down-staging before RC. It was not associated with better oncologic outcomes for patients with organ-confined bladder cancer.</p>\",\"PeriodicalId\":39147,\"journal\":{\"name\":\"Current Urology\",\"volume\":\"16 3\",\"pages\":\"142-146\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2022-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2c/16/curr-urol-16-142.PMC9527917.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Urology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CU9.0000000000000110\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/8/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CU9.0000000000000110","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/8/27 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Complete transurethral resection of bladder tumor before radical cystectomy is not a risk factor for organ-confined bladder cancer: A case-control study.
Objectives: To investigate the role of complete transurethral resection of bladder tumor (TURBT) before radical cystectomy (RC) for organ-confined bladder cancer.
Materials and methods: Data of patients who underwent RC in our center from January 2008 to December 2018 were retrospectively reviewed. Patients with >T2N0M0 disease and positive surgical margins and those who received neoadjuvant/adjuvant chemotherapy or radiotherapy were excluded. Complete TURBT was defined as no visible lesion under endoscopic examination after TURBT or in the bladder specimen after RC. Kaplan-Meier curves and log-rank tests assessed disease-free survival (DFS). Logistic and Cox regression analyses were performed to identify potential predictors.
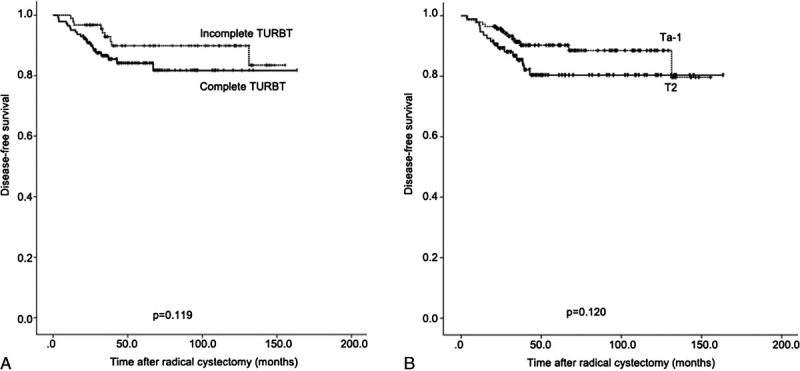
Results: A total of 236 patients were included in this review, including 207 males, with a median age of 61 years. The median tumor size was 3 cm, and a total of 94 patients had identified pathological T2 stage disease. Complete TURBT was correlated with tumor size (p = 0.041), histological variants (p = 0.026), and down-staging (p < 0.001). Tumor size, grade, and histological variants were independent predictors of complete TURBT. During a median follow-up of 42.7 months, 30 patients developed disease recurrence. Age and histological variants were independent predictors of DFS (p = 0.022 and 0.032, respectively), whereas complete TURBT was not an independent predictor of DFS (p = 0.156). Down-staging was not associated with survival outcome.
Conclusions: Complete TURBT was correlated with an increased rate of down-staging before RC. It was not associated with better oncologic outcomes for patients with organ-confined bladder cancer.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
