{"title":"急性脑损伤患者早期与晚期气管切开术:SET评分的重要性。","authors":"Saurav Shekhar, Raj Bahadur Singh, Ranjeet Rana De, Ritu Singh, Akhileshwar, Nitin Kumar","doi":"10.4103/aer.aer_22_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Patients with acute brain injury presents are unique subset of neurocritical care patients with its long-term functional prognosis difficult to determine. They often have long intensive care unit (ICU) stay and presents as challenge to decide when to transfer out of ICU. This prospective study aims to assess the benefits of early tracheostomy in terms of ICU-length of stay (ICU-LOS), number of days on ventilator (ventilator days), incidence of ventilator-associated pneumonia (VAP), and mortality rates.</p><p><strong>Materials and methods: </strong>After institutional ethical clearance, 80 patients were randomized into two groups: Group A, early tracheostomy group (tracheostomy within 3 days of intubation) and Group B, standard of care group (tracheostomy after 10 days of intubation: late tracheostomy). A cutoff of 10 in the SET score was used in predicting need of early tracheostomy; both groups were compared with respect to ICU-LOS, number of ventilator days (ventilation time), need of analgesia and sedation, incidence of VAP, and mortality data.</p><p><strong>Results: </strong>Both the groups were comparable in terms of demographic profile and various disease severity scores. ICU-LOS was 14.9 ± 3.6 days in Group A and 17.2 ± 4.6 in Group B. The number of days on ventilator and incidence of VAP was significantly lower in Group A as compared to Group B. There was significantly lower mortality in Group A subset of patients in ICU.</p><p><strong>Conclusion: </strong>SET score is a simple and reliable score with fair accuracy and high sensitivity and specificity in predicting need of tracheostomy in neurocritical patients. A cutoff of 10 in the score can be reliably used in predicting need of early tracheostomy as in few other studies. Early tracheostomy is clearly advantageous in neurocritical patients, but has no advantage in terms of long-term mortality rates.</p>","PeriodicalId":7798,"journal":{"name":"Anesthesia, Essays and Researches","volume":"16 1","pages":"7-11"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9558650/pdf/","citationCount":"1","resultStr":"{\"title\":\"Early versus Late Tracheostomy in Patients with Acute Brain Injury: Importance of SET Score.\",\"authors\":\"Saurav Shekhar, Raj Bahadur Singh, Ranjeet Rana De, Ritu Singh, Akhileshwar, Nitin Kumar\",\"doi\":\"10.4103/aer.aer_22_22\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Patients with acute brain injury presents are unique subset of neurocritical care patients with its long-term functional prognosis difficult to determine. They often have long intensive care unit (ICU) stay and presents as challenge to decide when to transfer out of ICU. This prospective study aims to assess the benefits of early tracheostomy in terms of ICU-length of stay (ICU-LOS), number of days on ventilator (ventilator days), incidence of ventilator-associated pneumonia (VAP), and mortality rates.</p><p><strong>Materials and methods: </strong>After institutional ethical clearance, 80 patients were randomized into two groups: Group A, early tracheostomy group (tracheostomy within 3 days of intubation) and Group B, standard of care group (tracheostomy after 10 days of intubation: late tracheostomy). A cutoff of 10 in the SET score was used in predicting need of early tracheostomy; both groups were compared with respect to ICU-LOS, number of ventilator days (ventilation time), need of analgesia and sedation, incidence of VAP, and mortality data.</p><p><strong>Results: </strong>Both the groups were comparable in terms of demographic profile and various disease severity scores. ICU-LOS was 14.9 ± 3.6 days in Group A and 17.2 ± 4.6 in Group B. The number of days on ventilator and incidence of VAP was significantly lower in Group A as compared to Group B. There was significantly lower mortality in Group A subset of patients in ICU.</p><p><strong>Conclusion: </strong>SET score is a simple and reliable score with fair accuracy and high sensitivity and specificity in predicting need of tracheostomy in neurocritical patients. A cutoff of 10 in the score can be reliably used in predicting need of early tracheostomy as in few other studies. Early tracheostomy is clearly advantageous in neurocritical patients, but has no advantage in terms of long-term mortality rates.</p>\",\"PeriodicalId\":7798,\"journal\":{\"name\":\"Anesthesia, Essays and Researches\",\"volume\":\"16 1\",\"pages\":\"7-11\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9558650/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anesthesia, Essays and Researches\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/aer.aer_22_22\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/5/31 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia, Essays and Researches","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/aer.aer_22_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/5/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
急性脑损伤患者是神经危重症患者中一个独特的亚群,其长期功能预后难以确定。他们通常在重症监护室(ICU)呆很长时间,对决定何时转出ICU提出了挑战。本前瞻性研究旨在评估早期气管切开术在icu -住院时间(ICU-LOS)、呼吸机使用天数(呼吸机天数)、呼吸机相关性肺炎(VAP)发生率和死亡率方面的益处。材料与方法:80例患者经机构伦理审查后随机分为A组(气管插管后3天内)和B组(气管插管后10天内)。SET评分10分的临界值用于预测早期气管切开术的需要;比较两组患者ICU-LOS、呼吸机天数(通气时间)、镇痛镇静需求、VAP发生率和死亡率数据。结果:两组在人口学特征和各种疾病严重程度评分方面具有可比性。ICU- los A组为14.9±3.6 d, b组为17.2±4.6 d, A组呼吸机天数和VAP发生率明显低于b组,A组患者在ICU的死亡率明显低于b组。结论:SET评分是预测神经危重症患者气管切开术需要的一种简便、可靠的评分方法,准确度较高,敏感性和特异性较高。分数中10分的分界点可以可靠地用于预测早期气管切开术的需要,这在其他研究中很少出现。早期气管切开术显然对神经危重症患者有利,但在长期死亡率方面没有优势。
Early versus Late Tracheostomy in Patients with Acute Brain Injury: Importance of SET Score.
Introduction: Patients with acute brain injury presents are unique subset of neurocritical care patients with its long-term functional prognosis difficult to determine. They often have long intensive care unit (ICU) stay and presents as challenge to decide when to transfer out of ICU. This prospective study aims to assess the benefits of early tracheostomy in terms of ICU-length of stay (ICU-LOS), number of days on ventilator (ventilator days), incidence of ventilator-associated pneumonia (VAP), and mortality rates.
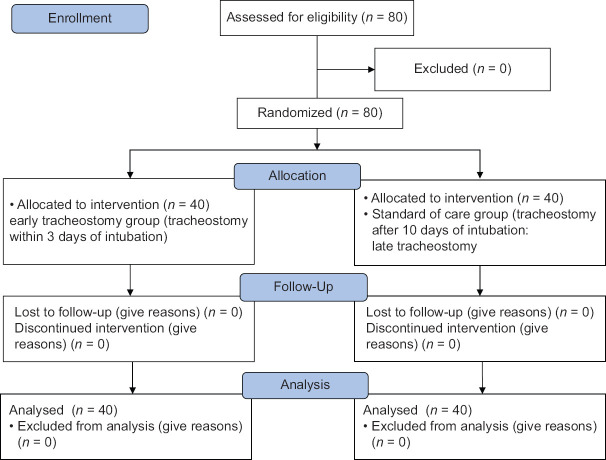
Materials and methods: After institutional ethical clearance, 80 patients were randomized into two groups: Group A, early tracheostomy group (tracheostomy within 3 days of intubation) and Group B, standard of care group (tracheostomy after 10 days of intubation: late tracheostomy). A cutoff of 10 in the SET score was used in predicting need of early tracheostomy; both groups were compared with respect to ICU-LOS, number of ventilator days (ventilation time), need of analgesia and sedation, incidence of VAP, and mortality data.
Results: Both the groups were comparable in terms of demographic profile and various disease severity scores. ICU-LOS was 14.9 ± 3.6 days in Group A and 17.2 ± 4.6 in Group B. The number of days on ventilator and incidence of VAP was significantly lower in Group A as compared to Group B. There was significantly lower mortality in Group A subset of patients in ICU.
Conclusion: SET score is a simple and reliable score with fair accuracy and high sensitivity and specificity in predicting need of tracheostomy in neurocritical patients. A cutoff of 10 in the score can be reliably used in predicting need of early tracheostomy as in few other studies. Early tracheostomy is clearly advantageous in neurocritical patients, but has no advantage in terms of long-term mortality rates.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
