{"title":"术中确定亚洲人髋部骨折股骨近端内钉术中预防股深动脉损伤的危险角度和安全距离。","authors":"Takehiro Kaneoka, Takashi Imagama, Manabu Yamamoto","doi":"10.5152/j.aott.2022.22061","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>During proximal femoral nailing, deep femoral artery injury, a rare condition, is often missed and found late, leading to intractable complications such as false aneurysm, hematoma, and anemia. We aimed to determine the novel indicators of the high-risk vertical range and axial angle for deep femoral artery injury that can be easily confirmed intraoperatively using fluoroscopy for hip fracture.</p><p><strong>Methods: </strong>In a single hospital, the lower extremity computed tomography angiographies of 88 patients (50 men and 38 women) were analyzed. A reference plane was defined as the femoral neck and shaft on the same straight line in the lateral view. Reference points were the lower end of the lesser trochanter and distal femur at 140 mm from the tip of the greater trochanter. To determine the high-risk angle for deep femoral artery injury based on the reference plane, the angle from the reference plane to the deep femoral artery (bone-arterial angle) and the shortest distance between the surfaces of the femur and the deep femoral artery (bone-artery distance) were measured at the lesser trochanter and the greater trochanter. We analyzed the bone-arterial angle and bone-artery distance values, their differences among the sexes, and their correlation with body height and body weight.</p><p><strong>Results: </strong>Overall, in the lesser trochanter, the mean bone-arterial angle and bone-artery distance were 19.2° ± 8.0° and 22.9 ± 4.7 mm, respectively. In the greater trochanter, the mean bone-arterial angle and bone-artery distance were -33.9° ± 17.0° and 11.3 ± 4.1 mm, respectively. The mean bone-artery distance of the lesser trochanter was significantly longer in men than in women (24.1 ± 4.5 mm and 21.4 ± 4.5 mm, respectively, P < 0.01), and for the lesser trochanter, positive correlations were found between body height and both bone- arterial angle and bone-artery distance (r=0.373, P < 0.001; and r=0.456, P < 0.0001, respectively), with body weight and bone-artery distance positively correlated (r=0.367, P < 0.001). At the greater trochanter, there were negative correlations between body height and bone-arterial angle (r=-0.5671, P < 0.0001), body weight, and bone-arterial angle (r=-0.338, P < 0.01).</p><p><strong>Conclusion: </strong>The knowledge of our reference plane and high-risk angles and distances allows surgeons to minimize the risk of deep femoral artery injury. These are easily confirmed intraoperatively using fluoroscopy, allowing surgeons to avoid maneuvering in the deep femoral artery range.</p><p><strong>Level of evidence: </strong>Level IV, Diagnostic Study.</p>","PeriodicalId":7097,"journal":{"name":"Acta orthopaedica et traumatologica turcica","volume":" ","pages":"300-305"},"PeriodicalIF":1.1000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bc/f6/aott-56-5-300.PMC9682588.pdf","citationCount":"0","resultStr":"{\"title\":\"Intraoperative determination of the risky angles and safe distances for preventing deep femoral artery injury during proximal femoral nailing for hip fractures in Asian people.\",\"authors\":\"Takehiro Kaneoka, Takashi Imagama, Manabu Yamamoto\",\"doi\":\"10.5152/j.aott.2022.22061\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>During proximal femoral nailing, deep femoral artery injury, a rare condition, is often missed and found late, leading to intractable complications such as false aneurysm, hematoma, and anemia. We aimed to determine the novel indicators of the high-risk vertical range and axial angle for deep femoral artery injury that can be easily confirmed intraoperatively using fluoroscopy for hip fracture.</p><p><strong>Methods: </strong>In a single hospital, the lower extremity computed tomography angiographies of 88 patients (50 men and 38 women) were analyzed. A reference plane was defined as the femoral neck and shaft on the same straight line in the lateral view. Reference points were the lower end of the lesser trochanter and distal femur at 140 mm from the tip of the greater trochanter. To determine the high-risk angle for deep femoral artery injury based on the reference plane, the angle from the reference plane to the deep femoral artery (bone-arterial angle) and the shortest distance between the surfaces of the femur and the deep femoral artery (bone-artery distance) were measured at the lesser trochanter and the greater trochanter. We analyzed the bone-arterial angle and bone-artery distance values, their differences among the sexes, and their correlation with body height and body weight.</p><p><strong>Results: </strong>Overall, in the lesser trochanter, the mean bone-arterial angle and bone-artery distance were 19.2° ± 8.0° and 22.9 ± 4.7 mm, respectively. In the greater trochanter, the mean bone-arterial angle and bone-artery distance were -33.9° ± 17.0° and 11.3 ± 4.1 mm, respectively. The mean bone-artery distance of the lesser trochanter was significantly longer in men than in women (24.1 ± 4.5 mm and 21.4 ± 4.5 mm, respectively, P < 0.01), and for the lesser trochanter, positive correlations were found between body height and both bone- arterial angle and bone-artery distance (r=0.373, P < 0.001; and r=0.456, P < 0.0001, respectively), with body weight and bone-artery distance positively correlated (r=0.367, P < 0.001). At the greater trochanter, there were negative correlations between body height and bone-arterial angle (r=-0.5671, P < 0.0001), body weight, and bone-arterial angle (r=-0.338, P < 0.01).</p><p><strong>Conclusion: </strong>The knowledge of our reference plane and high-risk angles and distances allows surgeons to minimize the risk of deep femoral artery injury. These are easily confirmed intraoperatively using fluoroscopy, allowing surgeons to avoid maneuvering in the deep femoral artery range.</p><p><strong>Level of evidence: </strong>Level IV, Diagnostic Study.</p>\",\"PeriodicalId\":7097,\"journal\":{\"name\":\"Acta orthopaedica et traumatologica turcica\",\"volume\":\" \",\"pages\":\"300-305\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2022-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bc/f6/aott-56-5-300.PMC9682588.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta orthopaedica et traumatologica turcica\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5152/j.aott.2022.22061\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta orthopaedica et traumatologica turcica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5152/j.aott.2022.22061","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
摘要
目的:股近端髓内钉术中,股深动脉损伤是一种罕见的情况,常被漏诊和发现较晚,导致假性动脉瘤、血肿、贫血等难治性并发症。我们的目的是确定股骨深动脉损伤的高危垂直范围和轴向角度的新指标,这些指标可以在术中通过髋部骨折的透视检查轻松确认。方法:对某医院88例患者(男50例,女38例)的下肢ct血管造影资料进行分析。参考平面定义为股骨颈和股骨轴在侧位视图中的同一直线上。参考点为距大转子尖端140 mm处的小转子下端和股骨远端。为了根据参考平面确定股深动脉损伤的高危角度,在小转子和大转子处测量参考平面到股深动脉的夹角(骨-动脉夹角)和股骨表面到股深动脉的最短距离(骨-动脉距离)。我们分析了骨动脉角和骨动脉距离值,它们的性别差异,以及它们与身高和体重的相关性。结果:总体而言,小转子骨动脉夹角和骨动脉距离的平均值分别为19.2°±8.0°和22.9±4.7 mm。大转子骨动脉夹角平均值为-33.9°±17.0°,骨动脉距离平均值为11.3±4.1 mm。男性小转子的平均骨动脉距离明显长于女性(分别为24.1±4.5 mm和21.4±4.5 mm, P < 0.01),而身高与小转子的骨动脉角和骨动脉距离均呈正相关(r=0.373, P < 0.001;和r=0.456, P < 0.0001),体重与骨动脉距离呈正相关(r=0.367, P < 0.001)。在大转子处,身高与骨动脉角呈负相关(r=-0.5671, P < 0.0001),体重与骨动脉角呈负相关(r=-0.338, P < 0.01)。结论:了解我们的参考平面和高危角度和距离可以使外科医生将股深动脉损伤的风险降至最低。术中使用透视检查很容易确认,允许外科医生避免在股深动脉范围内操作。证据等级:四级,诊断性研究。
Intraoperative determination of the risky angles and safe distances for preventing deep femoral artery injury during proximal femoral nailing for hip fractures in Asian people.
Objective: During proximal femoral nailing, deep femoral artery injury, a rare condition, is often missed and found late, leading to intractable complications such as false aneurysm, hematoma, and anemia. We aimed to determine the novel indicators of the high-risk vertical range and axial angle for deep femoral artery injury that can be easily confirmed intraoperatively using fluoroscopy for hip fracture.
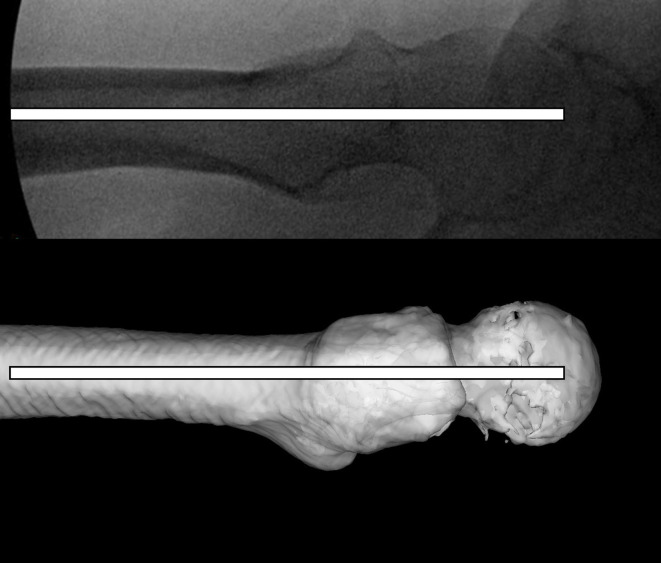
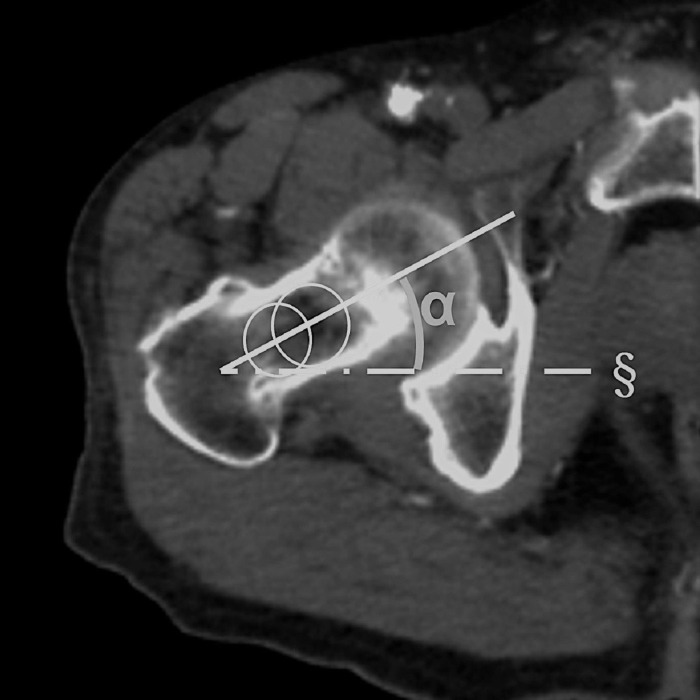
Methods: In a single hospital, the lower extremity computed tomography angiographies of 88 patients (50 men and 38 women) were analyzed. A reference plane was defined as the femoral neck and shaft on the same straight line in the lateral view. Reference points were the lower end of the lesser trochanter and distal femur at 140 mm from the tip of the greater trochanter. To determine the high-risk angle for deep femoral artery injury based on the reference plane, the angle from the reference plane to the deep femoral artery (bone-arterial angle) and the shortest distance between the surfaces of the femur and the deep femoral artery (bone-artery distance) were measured at the lesser trochanter and the greater trochanter. We analyzed the bone-arterial angle and bone-artery distance values, their differences among the sexes, and their correlation with body height and body weight.
Results: Overall, in the lesser trochanter, the mean bone-arterial angle and bone-artery distance were 19.2° ± 8.0° and 22.9 ± 4.7 mm, respectively. In the greater trochanter, the mean bone-arterial angle and bone-artery distance were -33.9° ± 17.0° and 11.3 ± 4.1 mm, respectively. The mean bone-artery distance of the lesser trochanter was significantly longer in men than in women (24.1 ± 4.5 mm and 21.4 ± 4.5 mm, respectively, P < 0.01), and for the lesser trochanter, positive correlations were found between body height and both bone- arterial angle and bone-artery distance (r=0.373, P < 0.001; and r=0.456, P < 0.0001, respectively), with body weight and bone-artery distance positively correlated (r=0.367, P < 0.001). At the greater trochanter, there were negative correlations between body height and bone-arterial angle (r=-0.5671, P < 0.0001), body weight, and bone-arterial angle (r=-0.338, P < 0.01).
Conclusion: The knowledge of our reference plane and high-risk angles and distances allows surgeons to minimize the risk of deep femoral artery injury. These are easily confirmed intraoperatively using fluoroscopy, allowing surgeons to avoid maneuvering in the deep femoral artery range.
期刊介绍:
Acta Orthopaedica et Traumatologica Turcica (AOTT) is an international, scientific, open access periodical published in accordance with independent, unbiased, and double-blinded peer-review principles. The journal is the official publication of the Turkish Association of Orthopaedics and Traumatology, and Turkish Society of Orthopaedics and Traumatology. It is published bimonthly in January, March, May, July, September, and November. The publication language of the journal is English.
The aim of the journal is to publish original studies of the highest scientific and clinical value in orthopedics, traumatology, and related disciplines. The scope of the journal includes but not limited to diagnostic, treatment, and prevention methods related to orthopedics and traumatology. Acta Orthopaedica et Traumatologica Turcica publishes clinical and basic research articles, case reports, personal clinical and technical notes, systematic reviews and meta-analyses and letters to the Editor. Proceedings of scientific meetings are also considered for publication.
The target audience of the journal includes healthcare professionals, physicians, and researchers who are interested or working in orthopedics and traumatology field, and related disciplines.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
