Simón Gundín, Juan Irure-Ventura, Esther Asensio, David Ramos, Michael Mahler, Victor Martínez-Taboada, Marcos López-Hoyos
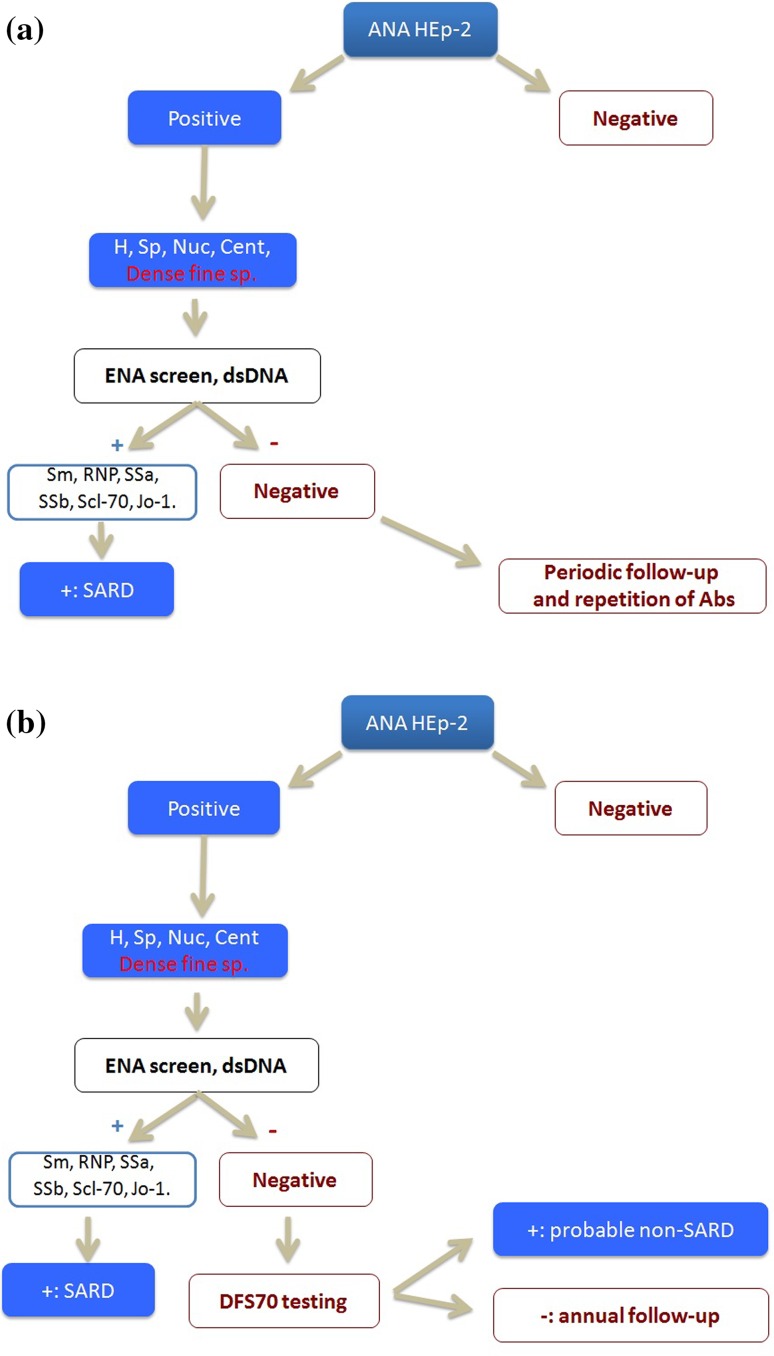
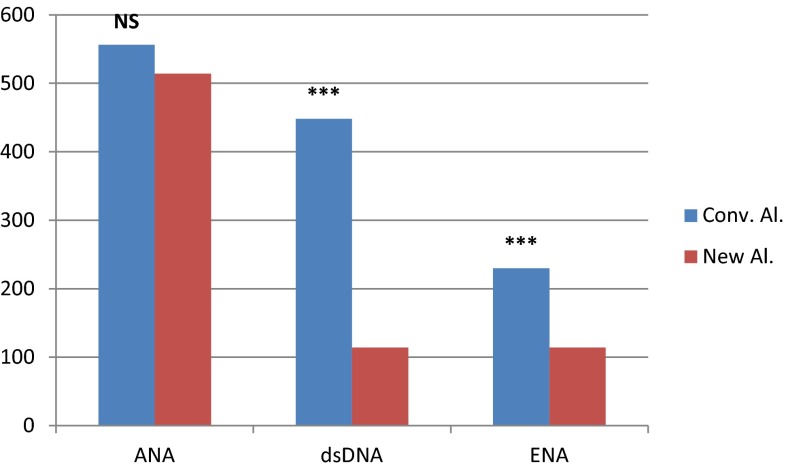
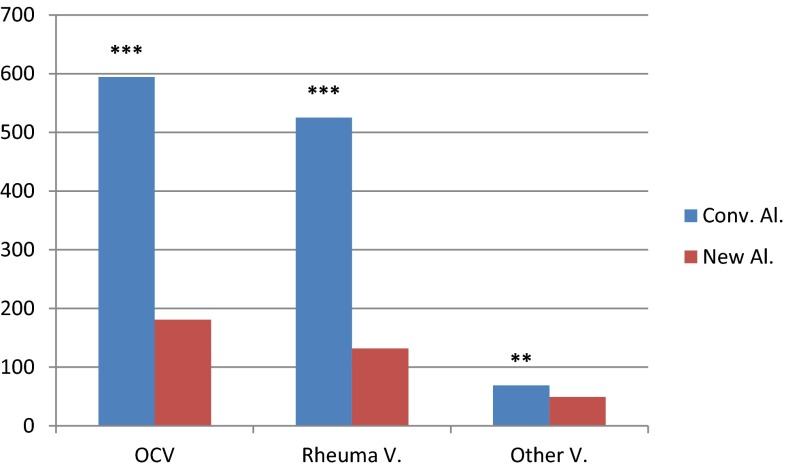
{"title":"在疑似与ana相关的自身免疫性风湿病患者中检测抗dfs70抗体具有成本效益。","authors":"Simón Gundín, Juan Irure-Ventura, Esther Asensio, David Ramos, Michael Mahler, Victor Martínez-Taboada, Marcos López-Hoyos","doi":"10.1007/s13317-016-0082-1","DOIUrl":null,"url":null,"abstract":"<p><p>The presence of antinuclear antibodies (ANA) is associated with a wide range of ANA-associated autoimmune rheumatic diseases (AARD). The most commonly method used for the detection of ANA is indirect immunofluorescence (IIF) on HEp-2 cells. This method is very sensitive but unspecific. As a consequence, ANA testing on HEp-2 substrates outside a proper clinical specialist framework may lead to inappropriate referrals to tertiary care specialists and, worst case inappropriate and potentially toxic therapy for the patient. Among ANA, isolated anti-DFS70 antibodies represent a potentially important biomarker that can be clinically used to discriminate AARD from non-AARD patients in ANA IIF positive individuals. Therefore, their presence may avoid unnecessary follow-up testing and referrals. In our study, we investigated if the implementation of a new ANA workup algorithm allowing for the identification of anti-DFS70 antibodies is cost-effective through the reduction of both unnecessary follow-up testing and outpatient clinic visits generated by the clinical suspicion of a potential AARD. None of the 181 patients included with a positive monospecific anti-DFS70 antibody result developed SARD during the follow-up period of 10 years. The reduction in number of tests after ANA and anti-DFS70 positive results was significant for anti-ENA (230 vs. 114 tests; p < 0.001) and anti-dsDNA antibodies (448 vs. 114 tests; p < 0.001). In addition, the outpatient clinic visits decreased by 70 % (p < 0.001). In total, the adoption of the new algorithm including anti-DFS70 antibody testing resulted in a cost saving of 60869.53 € for this pilot study. In conclusion, the use of anti-DFS70 antibodies was clearly cost-efficient in our setting. </p>","PeriodicalId":8655,"journal":{"name":"Auto-Immunity Highlights","volume":"7 1","pages":"10"},"PeriodicalIF":0.0000,"publicationDate":"2016-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s13317-016-0082-1","citationCount":"44","resultStr":"{\"title\":\"Measurement of anti-DFS70 antibodies in patients with ANA-associated autoimmune rheumatic diseases suspicion is cost-effective.\",\"authors\":\"Simón Gundín, Juan Irure-Ventura, Esther Asensio, David Ramos, Michael Mahler, Victor Martínez-Taboada, Marcos López-Hoyos\",\"doi\":\"10.1007/s13317-016-0082-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The presence of antinuclear antibodies (ANA) is associated with a wide range of ANA-associated autoimmune rheumatic diseases (AARD). The most commonly method used for the detection of ANA is indirect immunofluorescence (IIF) on HEp-2 cells. This method is very sensitive but unspecific. As a consequence, ANA testing on HEp-2 substrates outside a proper clinical specialist framework may lead to inappropriate referrals to tertiary care specialists and, worst case inappropriate and potentially toxic therapy for the patient. Among ANA, isolated anti-DFS70 antibodies represent a potentially important biomarker that can be clinically used to discriminate AARD from non-AARD patients in ANA IIF positive individuals. Therefore, their presence may avoid unnecessary follow-up testing and referrals. In our study, we investigated if the implementation of a new ANA workup algorithm allowing for the identification of anti-DFS70 antibodies is cost-effective through the reduction of both unnecessary follow-up testing and outpatient clinic visits generated by the clinical suspicion of a potential AARD. None of the 181 patients included with a positive monospecific anti-DFS70 antibody result developed SARD during the follow-up period of 10 years. The reduction in number of tests after ANA and anti-DFS70 positive results was significant for anti-ENA (230 vs. 114 tests; p < 0.001) and anti-dsDNA antibodies (448 vs. 114 tests; p < 0.001). In addition, the outpatient clinic visits decreased by 70 % (p < 0.001). In total, the adoption of the new algorithm including anti-DFS70 antibody testing resulted in a cost saving of 60869.53 € for this pilot study. In conclusion, the use of anti-DFS70 antibodies was clearly cost-efficient in our setting. </p>\",\"PeriodicalId\":8655,\"journal\":{\"name\":\"Auto-Immunity Highlights\",\"volume\":\"7 1\",\"pages\":\"10\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1007/s13317-016-0082-1\",\"citationCount\":\"44\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Auto-Immunity Highlights\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s13317-016-0082-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/7/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Auto-Immunity Highlights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s13317-016-0082-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/7/29 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Measurement of anti-DFS70 antibodies in patients with ANA-associated autoimmune rheumatic diseases suspicion is cost-effective.
The presence of antinuclear antibodies (ANA) is associated with a wide range of ANA-associated autoimmune rheumatic diseases (AARD). The most commonly method used for the detection of ANA is indirect immunofluorescence (IIF) on HEp-2 cells. This method is very sensitive but unspecific. As a consequence, ANA testing on HEp-2 substrates outside a proper clinical specialist framework may lead to inappropriate referrals to tertiary care specialists and, worst case inappropriate and potentially toxic therapy for the patient. Among ANA, isolated anti-DFS70 antibodies represent a potentially important biomarker that can be clinically used to discriminate AARD from non-AARD patients in ANA IIF positive individuals. Therefore, their presence may avoid unnecessary follow-up testing and referrals. In our study, we investigated if the implementation of a new ANA workup algorithm allowing for the identification of anti-DFS70 antibodies is cost-effective through the reduction of both unnecessary follow-up testing and outpatient clinic visits generated by the clinical suspicion of a potential AARD. None of the 181 patients included with a positive monospecific anti-DFS70 antibody result developed SARD during the follow-up period of 10 years. The reduction in number of tests after ANA and anti-DFS70 positive results was significant for anti-ENA (230 vs. 114 tests; p < 0.001) and anti-dsDNA antibodies (448 vs. 114 tests; p < 0.001). In addition, the outpatient clinic visits decreased by 70 % (p < 0.001). In total, the adoption of the new algorithm including anti-DFS70 antibody testing resulted in a cost saving of 60869.53 € for this pilot study. In conclusion, the use of anti-DFS70 antibodies was clearly cost-efficient in our setting.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
