Hai Chen, Pradeep N Modur, Niravkumar Barot, Paul C Van Ness, Mark A Agostini, Kan Ding, Puneet Gupta, Ryan Hays, Bruce Mickey
{"title":"术后癫痫复发的预测因素:颞部和颞外切除的纵向研究。","authors":"Hai Chen, Pradeep N Modur, Niravkumar Barot, Paul C Van Ness, Mark A Agostini, Kan Ding, Puneet Gupta, Ryan Hays, Bruce Mickey","doi":"10.1155/2016/7982494","DOIUrl":null,"url":null,"abstract":"<p><p>Objective. We investigated the longitudinal outcome of resective epilepsy surgery to identify the predictors of seizure recurrence. Materials and Methods. We retrospectively analyzed patients who underwent resections for intractable epilepsy over a period of 7 years. Multiple variables were investigated as potential predictors of seizure recurrence. The time to first postoperative seizure was evaluated using survival analysis and univariate analysis at annual intervals. Results. Among 70 patients, 54 (77%) had temporal and 16 (23%) had extratemporal resections. At last follow-up (mean 48 months; range 24-87 months), the outcome was Engel class I in 84% (n = 59) of patients. Seizure recurrence followed two patterns: recurrence was \"early\" (within 2 years) in 82% of patients, of whom 83% continued to have seizures despite optimum medical therapy; recurrence was \"late\" (after 2 years) in 18%, of whom 25% continued to have seizures subsequently. Among the variables of interest, only resection site and ictal EEG remained as independent predictors of seizure recurrence over the long term (p < 0.05). Extratemporal resection and discordance between ictal EEG and resection area were associated with 4.2-fold and 5.6-fold higher risk of seizure recurrence, respectively. Conclusions. Extratemporal epilepsy and uncertainty in ictal EEG localization are independent predictors of unfavorable outcome. Seizure recurrence within two years of surgery indicates poor long-term outcome. </p>","PeriodicalId":72948,"journal":{"name":"Epilepsy research and treatment","volume":"2016 ","pages":"7982494"},"PeriodicalIF":0.0000,"publicationDate":"2016-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2016/7982494","citationCount":"12","resultStr":"{\"title\":\"Predictors of Postoperative Seizure Recurrence: A Longitudinal Study of Temporal and Extratemporal Resections.\",\"authors\":\"Hai Chen, Pradeep N Modur, Niravkumar Barot, Paul C Van Ness, Mark A Agostini, Kan Ding, Puneet Gupta, Ryan Hays, Bruce Mickey\",\"doi\":\"10.1155/2016/7982494\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Objective. We investigated the longitudinal outcome of resective epilepsy surgery to identify the predictors of seizure recurrence. Materials and Methods. We retrospectively analyzed patients who underwent resections for intractable epilepsy over a period of 7 years. Multiple variables were investigated as potential predictors of seizure recurrence. The time to first postoperative seizure was evaluated using survival analysis and univariate analysis at annual intervals. Results. Among 70 patients, 54 (77%) had temporal and 16 (23%) had extratemporal resections. At last follow-up (mean 48 months; range 24-87 months), the outcome was Engel class I in 84% (n = 59) of patients. Seizure recurrence followed two patterns: recurrence was \\\"early\\\" (within 2 years) in 82% of patients, of whom 83% continued to have seizures despite optimum medical therapy; recurrence was \\\"late\\\" (after 2 years) in 18%, of whom 25% continued to have seizures subsequently. Among the variables of interest, only resection site and ictal EEG remained as independent predictors of seizure recurrence over the long term (p < 0.05). Extratemporal resection and discordance between ictal EEG and resection area were associated with 4.2-fold and 5.6-fold higher risk of seizure recurrence, respectively. Conclusions. Extratemporal epilepsy and uncertainty in ictal EEG localization are independent predictors of unfavorable outcome. Seizure recurrence within two years of surgery indicates poor long-term outcome. </p>\",\"PeriodicalId\":72948,\"journal\":{\"name\":\"Epilepsy research and treatment\",\"volume\":\"2016 \",\"pages\":\"7982494\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2016/7982494\",\"citationCount\":\"12\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Epilepsy research and treatment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2016/7982494\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/3/16 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Epilepsy research and treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2016/7982494","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/3/16 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Predictors of Postoperative Seizure Recurrence: A Longitudinal Study of Temporal and Extratemporal Resections.
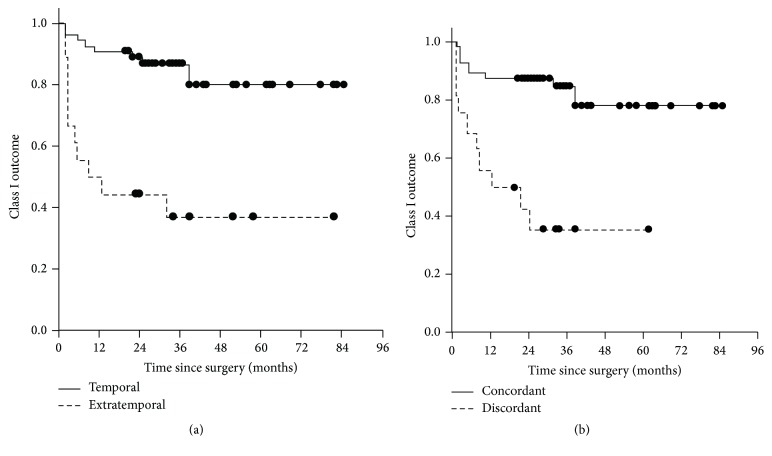
Objective. We investigated the longitudinal outcome of resective epilepsy surgery to identify the predictors of seizure recurrence. Materials and Methods. We retrospectively analyzed patients who underwent resections for intractable epilepsy over a period of 7 years. Multiple variables were investigated as potential predictors of seizure recurrence. The time to first postoperative seizure was evaluated using survival analysis and univariate analysis at annual intervals. Results. Among 70 patients, 54 (77%) had temporal and 16 (23%) had extratemporal resections. At last follow-up (mean 48 months; range 24-87 months), the outcome was Engel class I in 84% (n = 59) of patients. Seizure recurrence followed two patterns: recurrence was "early" (within 2 years) in 82% of patients, of whom 83% continued to have seizures despite optimum medical therapy; recurrence was "late" (after 2 years) in 18%, of whom 25% continued to have seizures subsequently. Among the variables of interest, only resection site and ictal EEG remained as independent predictors of seizure recurrence over the long term (p < 0.05). Extratemporal resection and discordance between ictal EEG and resection area were associated with 4.2-fold and 5.6-fold higher risk of seizure recurrence, respectively. Conclusions. Extratemporal epilepsy and uncertainty in ictal EEG localization are independent predictors of unfavorable outcome. Seizure recurrence within two years of surgery indicates poor long-term outcome.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
