Resa E Lewiss, Jessica Cook, Allison Sauler, Nicholas Avitabile, Nicole L Kaban, Jeffrey Rabrich, Turandot Saul, Sebastian D Siadecki, Dan Wiener
{"title":"工作流程工作组影响急诊医师对点护理超声文件和计费的依从性。","authors":"Resa E Lewiss, Jessica Cook, Allison Sauler, Nicholas Avitabile, Nicole L Kaban, Jeffrey Rabrich, Turandot Saul, Sebastian D Siadecki, Dan Wiener","doi":"10.1186/s13089-016-0041-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Emergency point-of-care ultrasound (POC u/s) is an example of a health information technology that improves patient care and time to correct diagnosis. POC u/s examinations should be documented, as they comprise an integral component of physician decision making. Incomplete documentation prevents coding, billing and physician group compensation for ultrasound-guided procedures and patient care. We aimed to assess the effect of directed education and personal feedback through a task force driven initiative to increase the number of POC u/s examinations documented and transferred to medical coders by emergency medicine physicians.</p><p><strong>Methods: </strong>Three months before a chosen go-live date, departmental leadership, the ultrasound division, and residents formed a task force. Barriers to documentation were identified through brain storming and email solicitation. The total number and application-specific POC u/s examinations performed and transferred to the healthcare record and medical coders were compared for the pre- and post-task force intervention periods. Chi square analysis was used to determine the difference between the number of POC u/s examinations reported before and after the intervention.</p><p><strong>Results: </strong>A total of 1652 POC u/s examinations were reported during the study period. Successful reporting to the patient care chart and medical coders increased from 41 % pre-task force intervention to 63 % post-intervention (p value 0.000). The number of scans performed during the 3-month periods (pre-intervetion, post-intervention 0-3 months, post-intervention 3-6 months) was similar (521, 594 and 537). When analyzed by specific application, the majority showed a statistically significant increase in the percentage of examinations reported, including those most critical for patient care decision making: (EFAST (41 vs. 64 %), vascular access (26 vs. 61 %), and cardiac (43 vs. 72 %); and those most commonly performed: biliary (44 vs. 61 %) and pelvic (60 vs. 66 %). Of the POC u/s studies coded and reported for reimbursement, 15.9 % were billed before intervention and 32 % were billed after intervention (p value: 0.000).</p><p><strong>Conclusions: </strong>The formation of a workflow solution task force positively affected emergency physician compliance with POC u/s documentation for coding and billing over a 6-month period. Further investigation should assess the long-term effect of the intervention and whether this translates into increased revenue to the department.</p>","PeriodicalId":46598,"journal":{"name":"Critical Ultrasound Journal","volume":"8 1","pages":"5"},"PeriodicalIF":3.6000,"publicationDate":"2016-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13089-016-0041-0","citationCount":"17","resultStr":"{\"title\":\"A workflow task force affects emergency physician compliance for point-of-care ultrasound documentation and billing.\",\"authors\":\"Resa E Lewiss, Jessica Cook, Allison Sauler, Nicholas Avitabile, Nicole L Kaban, Jeffrey Rabrich, Turandot Saul, Sebastian D Siadecki, Dan Wiener\",\"doi\":\"10.1186/s13089-016-0041-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Emergency point-of-care ultrasound (POC u/s) is an example of a health information technology that improves patient care and time to correct diagnosis. POC u/s examinations should be documented, as they comprise an integral component of physician decision making. Incomplete documentation prevents coding, billing and physician group compensation for ultrasound-guided procedures and patient care. We aimed to assess the effect of directed education and personal feedback through a task force driven initiative to increase the number of POC u/s examinations documented and transferred to medical coders by emergency medicine physicians.</p><p><strong>Methods: </strong>Three months before a chosen go-live date, departmental leadership, the ultrasound division, and residents formed a task force. Barriers to documentation were identified through brain storming and email solicitation. The total number and application-specific POC u/s examinations performed and transferred to the healthcare record and medical coders were compared for the pre- and post-task force intervention periods. Chi square analysis was used to determine the difference between the number of POC u/s examinations reported before and after the intervention.</p><p><strong>Results: </strong>A total of 1652 POC u/s examinations were reported during the study period. Successful reporting to the patient care chart and medical coders increased from 41 % pre-task force intervention to 63 % post-intervention (p value 0.000). The number of scans performed during the 3-month periods (pre-intervetion, post-intervention 0-3 months, post-intervention 3-6 months) was similar (521, 594 and 537). When analyzed by specific application, the majority showed a statistically significant increase in the percentage of examinations reported, including those most critical for patient care decision making: (EFAST (41 vs. 64 %), vascular access (26 vs. 61 %), and cardiac (43 vs. 72 %); and those most commonly performed: biliary (44 vs. 61 %) and pelvic (60 vs. 66 %). Of the POC u/s studies coded and reported for reimbursement, 15.9 % were billed before intervention and 32 % were billed after intervention (p value: 0.000).</p><p><strong>Conclusions: </strong>The formation of a workflow solution task force positively affected emergency physician compliance with POC u/s documentation for coding and billing over a 6-month period. Further investigation should assess the long-term effect of the intervention and whether this translates into increased revenue to the department.</p>\",\"PeriodicalId\":46598,\"journal\":{\"name\":\"Critical Ultrasound Journal\",\"volume\":\"8 1\",\"pages\":\"5\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2016-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s13089-016-0041-0\",\"citationCount\":\"17\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Ultrasound Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13089-016-0041-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/5/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-016-0041-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/5/20 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
A workflow task force affects emergency physician compliance for point-of-care ultrasound documentation and billing.
Background: Emergency point-of-care ultrasound (POC u/s) is an example of a health information technology that improves patient care and time to correct diagnosis. POC u/s examinations should be documented, as they comprise an integral component of physician decision making. Incomplete documentation prevents coding, billing and physician group compensation for ultrasound-guided procedures and patient care. We aimed to assess the effect of directed education and personal feedback through a task force driven initiative to increase the number of POC u/s examinations documented and transferred to medical coders by emergency medicine physicians.
Methods: Three months before a chosen go-live date, departmental leadership, the ultrasound division, and residents formed a task force. Barriers to documentation were identified through brain storming and email solicitation. The total number and application-specific POC u/s examinations performed and transferred to the healthcare record and medical coders were compared for the pre- and post-task force intervention periods. Chi square analysis was used to determine the difference between the number of POC u/s examinations reported before and after the intervention.
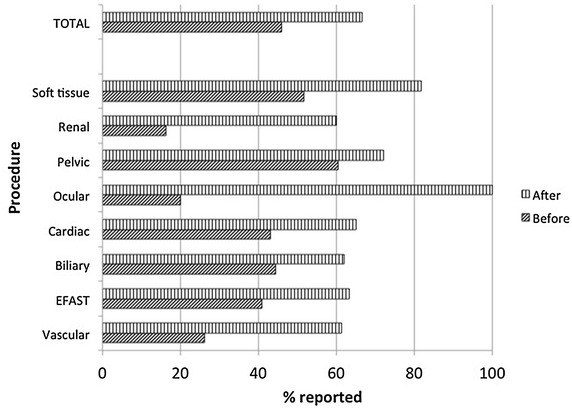
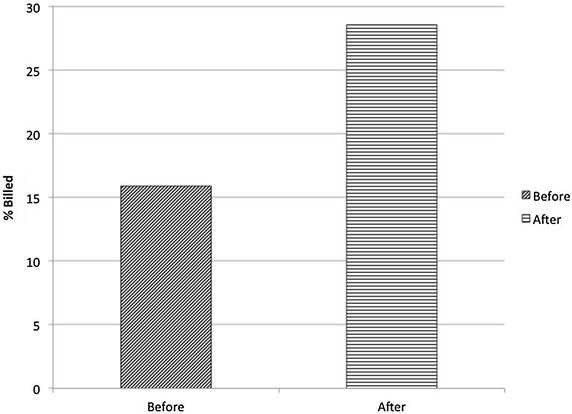
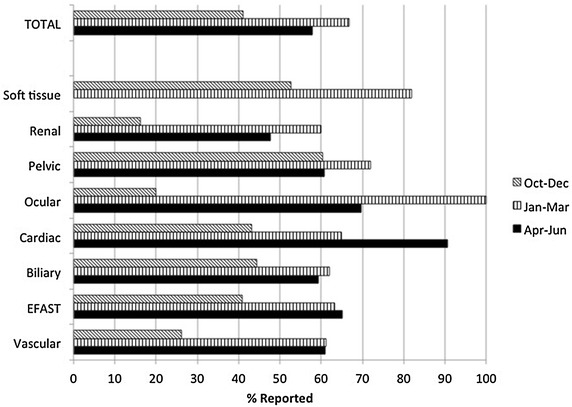
Results: A total of 1652 POC u/s examinations were reported during the study period. Successful reporting to the patient care chart and medical coders increased from 41 % pre-task force intervention to 63 % post-intervention (p value 0.000). The number of scans performed during the 3-month periods (pre-intervetion, post-intervention 0-3 months, post-intervention 3-6 months) was similar (521, 594 and 537). When analyzed by specific application, the majority showed a statistically significant increase in the percentage of examinations reported, including those most critical for patient care decision making: (EFAST (41 vs. 64 %), vascular access (26 vs. 61 %), and cardiac (43 vs. 72 %); and those most commonly performed: biliary (44 vs. 61 %) and pelvic (60 vs. 66 %). Of the POC u/s studies coded and reported for reimbursement, 15.9 % were billed before intervention and 32 % were billed after intervention (p value: 0.000).
Conclusions: The formation of a workflow solution task force positively affected emergency physician compliance with POC u/s documentation for coding and billing over a 6-month period. Further investigation should assess the long-term effect of the intervention and whether this translates into increased revenue to the department.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
