{"title":"透析钠梯度:液体超载的可改变危险因素。","authors":"Emilie Trinh, Catherine Weber","doi":"10.1159/000453674","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Fluid overload in patients on conventional hemodialysis is a frequent complication, associated with increased cardiovascular morbidity and mortality. The dialysate sodium prescription is a potential modifiable risk factor. Our primary objective was to describe associations between dialysate-to-serum sodium gradient and parameters of fluid status. A secondary objective was to evaluate the 6-month risk of hospitalization and mortality in relation to sodium gradient.</p><p><strong>Methods: </strong>We performed a cross-sectional study of 110 prevalent conventional hemodialysis patients at a single center. The associations of sodium gradient with interdialytic weight gain index (IDWG%), ultrafiltration (UF) rate, and blood pressure (BP) were analyzed.</p><p><strong>Results: </strong>The mean serum sodium gradient was 4.6 ± 3.6 mEq/L. There was a direct correlation between sodium gradient and IDWG% (<i>r</i> = 0.48, <i>p</i> < 0.01) as well as UF rate (<i>r</i> = 0.44, <i>p</i> < 0.01). In a logistic regression model, a 1 mEq/L higher sodium gradient was associated with increased risk of IDWG% >3% (OR 1.33, <i>p</i> < 0.01) and increased risk of UF rate >10 mL/kg/h (OR 1.16, <i>p</i> = 0.03), but there were no associations with intradialytic hypotension, intradialytic hypertension or BP. No significant differences were found with 6-month hospitalization or mortality risk in relation to sodium gradient.</p><p><strong>Conclusion: </strong>A higher sodium gradient was associated with significant increases in IDWG and UF rates, known to be associated with poor outcomes, but was not associated with intradialytic hypotension. Individualizing the dialysate sodium prescription to minimize sodium gap may lead to less fluid overload in conventional hemodialysis patients.</p>","PeriodicalId":56356,"journal":{"name":"Nephron Extra","volume":"7 1","pages":"10-17"},"PeriodicalIF":0.0000,"publicationDate":"2017-02-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000453674","citationCount":"10","resultStr":"{\"title\":\"The Dialysis Sodium Gradient: A Modifiable Risk Factor for Fluid Overload.\",\"authors\":\"Emilie Trinh, Catherine Weber\",\"doi\":\"10.1159/000453674\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Fluid overload in patients on conventional hemodialysis is a frequent complication, associated with increased cardiovascular morbidity and mortality. The dialysate sodium prescription is a potential modifiable risk factor. Our primary objective was to describe associations between dialysate-to-serum sodium gradient and parameters of fluid status. A secondary objective was to evaluate the 6-month risk of hospitalization and mortality in relation to sodium gradient.</p><p><strong>Methods: </strong>We performed a cross-sectional study of 110 prevalent conventional hemodialysis patients at a single center. The associations of sodium gradient with interdialytic weight gain index (IDWG%), ultrafiltration (UF) rate, and blood pressure (BP) were analyzed.</p><p><strong>Results: </strong>The mean serum sodium gradient was 4.6 ± 3.6 mEq/L. There was a direct correlation between sodium gradient and IDWG% (<i>r</i> = 0.48, <i>p</i> < 0.01) as well as UF rate (<i>r</i> = 0.44, <i>p</i> < 0.01). In a logistic regression model, a 1 mEq/L higher sodium gradient was associated with increased risk of IDWG% >3% (OR 1.33, <i>p</i> < 0.01) and increased risk of UF rate >10 mL/kg/h (OR 1.16, <i>p</i> = 0.03), but there were no associations with intradialytic hypotension, intradialytic hypertension or BP. No significant differences were found with 6-month hospitalization or mortality risk in relation to sodium gradient.</p><p><strong>Conclusion: </strong>A higher sodium gradient was associated with significant increases in IDWG and UF rates, known to be associated with poor outcomes, but was not associated with intradialytic hypotension. Individualizing the dialysate sodium prescription to minimize sodium gap may lead to less fluid overload in conventional hemodialysis patients.</p>\",\"PeriodicalId\":56356,\"journal\":{\"name\":\"Nephron Extra\",\"volume\":\"7 1\",\"pages\":\"10-17\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-02-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1159/000453674\",\"citationCount\":\"10\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nephron Extra\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000453674\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nephron Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000453674","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 10
摘要
背景:常规血液透析患者的体液超载是一种常见的并发症,与心血管发病率和死亡率增加有关。透析液钠处方是一个潜在的可改变的危险因素。我们的主要目的是描述透析液-血清钠梯度和流体状态参数之间的关系。次要目的是评估与钠梯度相关的6个月住院风险和死亡率。方法:我们在单一中心对110例流行的常规血液透析患者进行了横断面研究。分析了钠梯度与透析间期体重增加指数(IDWG%)、超滤率(UF)和血压(BP)的关系。结果:平均血清钠梯度为4.6±3.6 mEq/L。钠梯度与IDWG% (r = 0.48, p < 0.01)和UF率(r = 0.44, p < 0.01)有直接关系。在logistic回归模型中,1 mEq/L高钠梯度与IDWG风险增加% >3% (OR 1.33, p < 0.01)和UF率风险增加>10 mL/kg/h (OR 1.16, p = 0.03)相关,但与分析性低血压、分析性高血压或BP无关。钠梯度与6个月住院或死亡风险没有显著差异。结论:较高的钠梯度与IDWG和UF率的显著增加相关,已知与不良预后相关,但与溶性低血压无关。个体化透析钠处方以减少钠间隙可能会减少常规血液透析患者的液体过载。
The Dialysis Sodium Gradient: A Modifiable Risk Factor for Fluid Overload.
Background: Fluid overload in patients on conventional hemodialysis is a frequent complication, associated with increased cardiovascular morbidity and mortality. The dialysate sodium prescription is a potential modifiable risk factor. Our primary objective was to describe associations between dialysate-to-serum sodium gradient and parameters of fluid status. A secondary objective was to evaluate the 6-month risk of hospitalization and mortality in relation to sodium gradient.
Methods: We performed a cross-sectional study of 110 prevalent conventional hemodialysis patients at a single center. The associations of sodium gradient with interdialytic weight gain index (IDWG%), ultrafiltration (UF) rate, and blood pressure (BP) were analyzed.
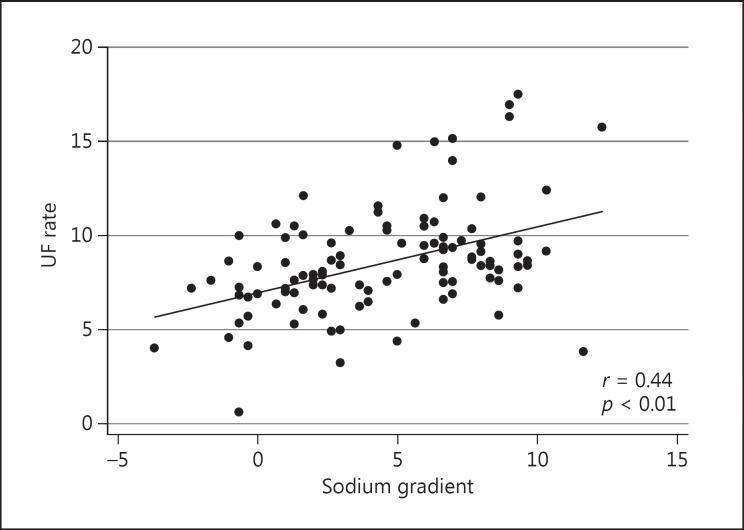
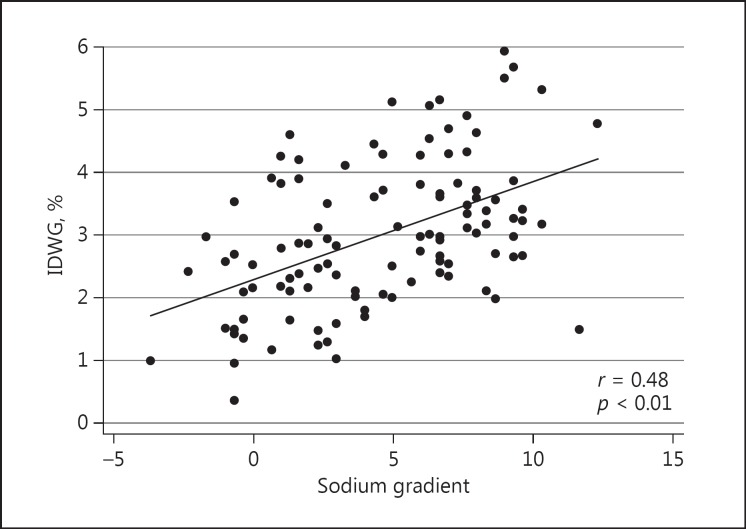
Results: The mean serum sodium gradient was 4.6 ± 3.6 mEq/L. There was a direct correlation between sodium gradient and IDWG% (r = 0.48, p < 0.01) as well as UF rate (r = 0.44, p < 0.01). In a logistic regression model, a 1 mEq/L higher sodium gradient was associated with increased risk of IDWG% >3% (OR 1.33, p < 0.01) and increased risk of UF rate >10 mL/kg/h (OR 1.16, p = 0.03), but there were no associations with intradialytic hypotension, intradialytic hypertension or BP. No significant differences were found with 6-month hospitalization or mortality risk in relation to sodium gradient.
Conclusion: A higher sodium gradient was associated with significant increases in IDWG and UF rates, known to be associated with poor outcomes, but was not associated with intradialytic hypotension. Individualizing the dialysate sodium prescription to minimize sodium gap may lead to less fluid overload in conventional hemodialysis patients.
期刊介绍:
An open-access subjournal to Nephron. ''Nephron EXTRA'' publishes additional high-quality articles that cannot be published in the main journal ''Nephron'' due to space limitations.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
