Feryal Abbas Ibrahim Hilmi, Ahmad Al-Sabbagh, Dina Sameh Soliman, Hesham Al Sabah, Omar Mohammad Ismail, Mohamed Yassin, Halima El-Omri
{"title":"急性髓系白血病伴Inv(16)(p13q22)伴隐蔽性全身肥大细胞增多症:病例报告及文献复习","authors":"Feryal Abbas Ibrahim Hilmi, Ahmad Al-Sabbagh, Dina Sameh Soliman, Hesham Al Sabah, Omar Mohammad Ismail, Mohamed Yassin, Halima El-Omri","doi":"10.1177/1179545X17700858","DOIUrl":null,"url":null,"abstract":"<p><p>Systemic mastocytosis (SM) is a condition associated with clonal neoplastic proliferation of mast cells. In up to 40% of systemic mastocytosis cases, an associated clonal hematological disease of non-mast cell lineage, such as acute myeloid leukemia (AML), is diagnosed before, simultaneously with, or after the diagnosis of SM. Herein, we report a case of a 30-year-old man diagnosed with AML with inv(16) (p13;q22) CBFB:MYH11. Associated mastocytosis was not noted at diagnosis and was only detected in the bone marrow at time of remission after successful chemotherapy. The diagnosis of mastocytosis was based on the demonstration of a multifocal dense mast cell infiltrate in the marrow biopsy with aberrant immunophenotype, with coexpression of tryptase, CD117, and CD25. The mast cells showed atypical morphology mostly with irregular nuclear contour, bilobed or multilobed nuclei with cytoplasmic hypogranulation or irregular metachromatic granule distribution, and some cells with eccentric nucleus or spindle shape. Reexamination of the pretherapeutic bone marrow with immunostain for tryptase and CD25 revealed that mastocytosis was present from the start but masked by extensive blast proliferation. This case indicates that mast cell infiltrates are sometimes underappreciated at the original diagnosis of AML with inv(16) and that the concurrent diagnosis of SM with AML requires a high index of suspicion supported with comprehensive morphologic and immunohistochemical evaluation for a neoplastic mast cell proliferation.</p>","PeriodicalId":43083,"journal":{"name":"Clinical Medicine Insights-Blood Disorders","volume":"10 ","pages":"1179545X17700858"},"PeriodicalIF":3.0000,"publicationDate":"2017-03-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179545X17700858","citationCount":"3","resultStr":"{\"title\":\"Acute Myeloid Leukemia With Inv(16)(p13q22) Associated With Hidden Systemic Mastocytosis: Case Report and Review of Literature.\",\"authors\":\"Feryal Abbas Ibrahim Hilmi, Ahmad Al-Sabbagh, Dina Sameh Soliman, Hesham Al Sabah, Omar Mohammad Ismail, Mohamed Yassin, Halima El-Omri\",\"doi\":\"10.1177/1179545X17700858\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Systemic mastocytosis (SM) is a condition associated with clonal neoplastic proliferation of mast cells. In up to 40% of systemic mastocytosis cases, an associated clonal hematological disease of non-mast cell lineage, such as acute myeloid leukemia (AML), is diagnosed before, simultaneously with, or after the diagnosis of SM. Herein, we report a case of a 30-year-old man diagnosed with AML with inv(16) (p13;q22) CBFB:MYH11. Associated mastocytosis was not noted at diagnosis and was only detected in the bone marrow at time of remission after successful chemotherapy. The diagnosis of mastocytosis was based on the demonstration of a multifocal dense mast cell infiltrate in the marrow biopsy with aberrant immunophenotype, with coexpression of tryptase, CD117, and CD25. The mast cells showed atypical morphology mostly with irregular nuclear contour, bilobed or multilobed nuclei with cytoplasmic hypogranulation or irregular metachromatic granule distribution, and some cells with eccentric nucleus or spindle shape. Reexamination of the pretherapeutic bone marrow with immunostain for tryptase and CD25 revealed that mastocytosis was present from the start but masked by extensive blast proliferation. This case indicates that mast cell infiltrates are sometimes underappreciated at the original diagnosis of AML with inv(16) and that the concurrent diagnosis of SM with AML requires a high index of suspicion supported with comprehensive morphologic and immunohistochemical evaluation for a neoplastic mast cell proliferation.</p>\",\"PeriodicalId\":43083,\"journal\":{\"name\":\"Clinical Medicine Insights-Blood Disorders\",\"volume\":\"10 \",\"pages\":\"1179545X17700858\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2017-03-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179545X17700858\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights-Blood Disorders\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179545X17700858\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Blood Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179545X17700858","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Acute Myeloid Leukemia With Inv(16)(p13q22) Associated With Hidden Systemic Mastocytosis: Case Report and Review of Literature.
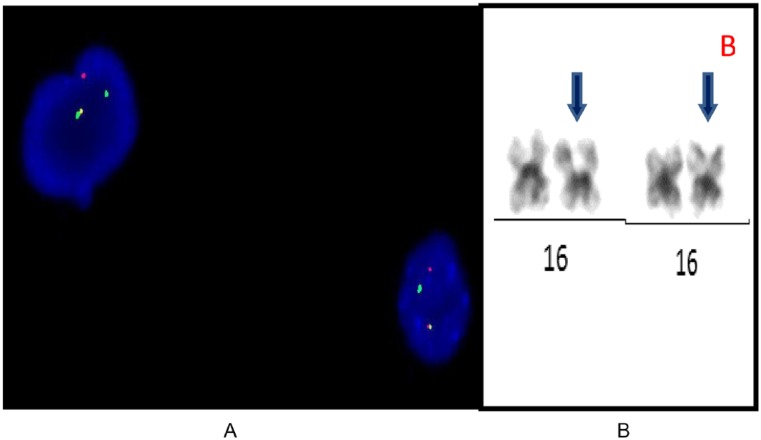
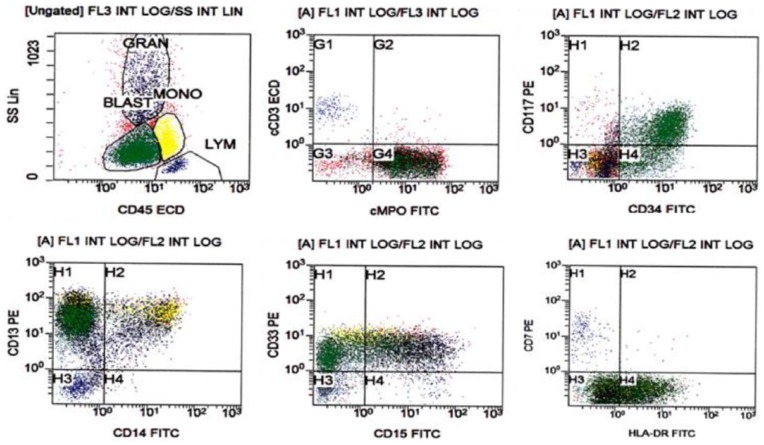
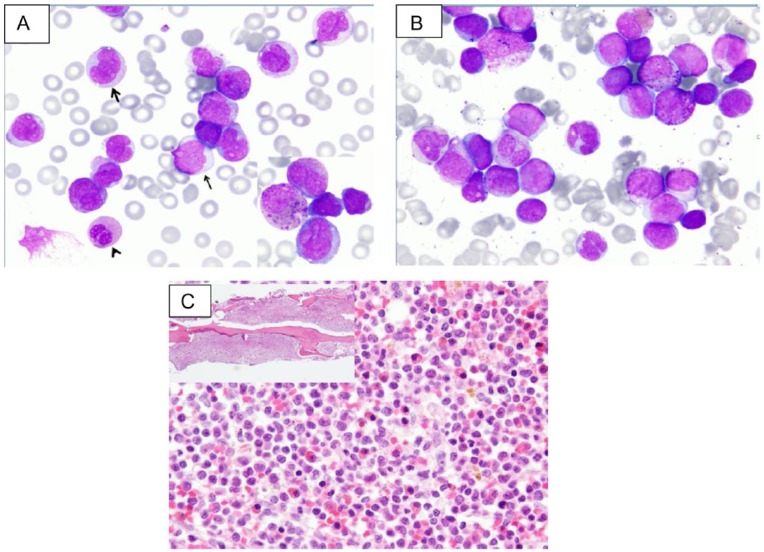
Systemic mastocytosis (SM) is a condition associated with clonal neoplastic proliferation of mast cells. In up to 40% of systemic mastocytosis cases, an associated clonal hematological disease of non-mast cell lineage, such as acute myeloid leukemia (AML), is diagnosed before, simultaneously with, or after the diagnosis of SM. Herein, we report a case of a 30-year-old man diagnosed with AML with inv(16) (p13;q22) CBFB:MYH11. Associated mastocytosis was not noted at diagnosis and was only detected in the bone marrow at time of remission after successful chemotherapy. The diagnosis of mastocytosis was based on the demonstration of a multifocal dense mast cell infiltrate in the marrow biopsy with aberrant immunophenotype, with coexpression of tryptase, CD117, and CD25. The mast cells showed atypical morphology mostly with irregular nuclear contour, bilobed or multilobed nuclei with cytoplasmic hypogranulation or irregular metachromatic granule distribution, and some cells with eccentric nucleus or spindle shape. Reexamination of the pretherapeutic bone marrow with immunostain for tryptase and CD25 revealed that mastocytosis was present from the start but masked by extensive blast proliferation. This case indicates that mast cell infiltrates are sometimes underappreciated at the original diagnosis of AML with inv(16) and that the concurrent diagnosis of SM with AML requires a high index of suspicion supported with comprehensive morphologic and immunohistochemical evaluation for a neoplastic mast cell proliferation.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
