Jesper Weile, Klaus Nielsen, Stine C Primdahl, Christian A Frederiksen, Christian B Laursen, Erik Sloth, Hans Kirkegaard
{"title":"超声检查在创伤:全国范围的横断面调查。","authors":"Jesper Weile, Klaus Nielsen, Stine C Primdahl, Christian A Frederiksen, Christian B Laursen, Erik Sloth, Hans Kirkegaard","doi":"10.1186/s13089-017-0071-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Focused Assessment with Sonography in Trauma (FAST) protocol is considered beneficial in emergent evaluation of trauma patients with blunt or penetrating injury and has become integrated into the Advanced Trauma Life Support (ATLS) protocol. No guidelines exist as to the use of ultrasonography in trauma in Denmark. We aimed to determine the current use of ultrasonography for assessing trauma patients in Denmark.</p><p><strong>Methods: </strong>We conducted a nation-wide cross-sectional investigation of ultrasonography usage in trauma care. The first phase consisted of an Internet-based investigation of existing guidelines, and the second phase was a series of structured interviews of orthopedic surgeons, anesthesiologists, and radiologists on call in all hospitals receiving traumatized patients in Denmark.</p><p><strong>Results: </strong>Guidelines were obtained from all 22 hospitals receiving traumatized patients in Denmark. Twenty-one (95.5%) of the guidelines included and recommended FAST as part of trauma assessment. The recommended person to perform the examination was the radiologist in n = 11 (50.0%), the surgeon in n = 6 (27.3%), the anesthesiologist in n = 1 (4.5%), and unspecified in n = 3 (13.6%) facilities. FAST indications varied between circulatory instability n = 8 (36.4%), team leader's discretion n = 6 (27.3%), abdominal trauma n = 3 (13.6%), and not specified n = 6 (27.3%). Telephone interviews revealed that exams were always n = 8 (36.4%) or often n = 4 (18.2%) registered in the patients' charts. The remaining n = 10 (45.5%) facilities either never registered n = 2 (9.1%), it was not possible to register n = 1 (4.5%), or unknown by the trauma leaders n = 7 (31.8%). Images were often stored in n = 1 (4.5%), never stored in n = 10 (45.5%), not possible to store in n = 2 (9.1%), and unknown in n = 9 (40.9%) facilities.</p><p><strong>Conclusion: </strong>Ultrasonography was used in a non-uniform fashion by multiple specialties in Danish trauma facilities. Very few images from FAST examinations were stored and documentation was scanty. National guidelines on application and documentation of ultrasonography in trauma are called for.</p>","PeriodicalId":46598,"journal":{"name":"Critical Ultrasound Journal","volume":"9 1","pages":"16"},"PeriodicalIF":3.6000,"publicationDate":"2017-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13089-017-0071-2","citationCount":"6","resultStr":"{\"title\":\"Ultrasonography in trauma: a nation-wide cross-sectional investigation.\",\"authors\":\"Jesper Weile, Klaus Nielsen, Stine C Primdahl, Christian A Frederiksen, Christian B Laursen, Erik Sloth, Hans Kirkegaard\",\"doi\":\"10.1186/s13089-017-0071-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The Focused Assessment with Sonography in Trauma (FAST) protocol is considered beneficial in emergent evaluation of trauma patients with blunt or penetrating injury and has become integrated into the Advanced Trauma Life Support (ATLS) protocol. No guidelines exist as to the use of ultrasonography in trauma in Denmark. We aimed to determine the current use of ultrasonography for assessing trauma patients in Denmark.</p><p><strong>Methods: </strong>We conducted a nation-wide cross-sectional investigation of ultrasonography usage in trauma care. The first phase consisted of an Internet-based investigation of existing guidelines, and the second phase was a series of structured interviews of orthopedic surgeons, anesthesiologists, and radiologists on call in all hospitals receiving traumatized patients in Denmark.</p><p><strong>Results: </strong>Guidelines were obtained from all 22 hospitals receiving traumatized patients in Denmark. Twenty-one (95.5%) of the guidelines included and recommended FAST as part of trauma assessment. The recommended person to perform the examination was the radiologist in n = 11 (50.0%), the surgeon in n = 6 (27.3%), the anesthesiologist in n = 1 (4.5%), and unspecified in n = 3 (13.6%) facilities. FAST indications varied between circulatory instability n = 8 (36.4%), team leader's discretion n = 6 (27.3%), abdominal trauma n = 3 (13.6%), and not specified n = 6 (27.3%). Telephone interviews revealed that exams were always n = 8 (36.4%) or often n = 4 (18.2%) registered in the patients' charts. The remaining n = 10 (45.5%) facilities either never registered n = 2 (9.1%), it was not possible to register n = 1 (4.5%), or unknown by the trauma leaders n = 7 (31.8%). Images were often stored in n = 1 (4.5%), never stored in n = 10 (45.5%), not possible to store in n = 2 (9.1%), and unknown in n = 9 (40.9%) facilities.</p><p><strong>Conclusion: </strong>Ultrasonography was used in a non-uniform fashion by multiple specialties in Danish trauma facilities. Very few images from FAST examinations were stored and documentation was scanty. National guidelines on application and documentation of ultrasonography in trauma are called for.</p>\",\"PeriodicalId\":46598,\"journal\":{\"name\":\"Critical Ultrasound Journal\",\"volume\":\"9 1\",\"pages\":\"16\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2017-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s13089-017-0071-2\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Ultrasound Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13089-017-0071-2\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/6/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-017-0071-2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/6/20 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Ultrasonography in trauma: a nation-wide cross-sectional investigation.
Background: The Focused Assessment with Sonography in Trauma (FAST) protocol is considered beneficial in emergent evaluation of trauma patients with blunt or penetrating injury and has become integrated into the Advanced Trauma Life Support (ATLS) protocol. No guidelines exist as to the use of ultrasonography in trauma in Denmark. We aimed to determine the current use of ultrasonography for assessing trauma patients in Denmark.
Methods: We conducted a nation-wide cross-sectional investigation of ultrasonography usage in trauma care. The first phase consisted of an Internet-based investigation of existing guidelines, and the second phase was a series of structured interviews of orthopedic surgeons, anesthesiologists, and radiologists on call in all hospitals receiving traumatized patients in Denmark.
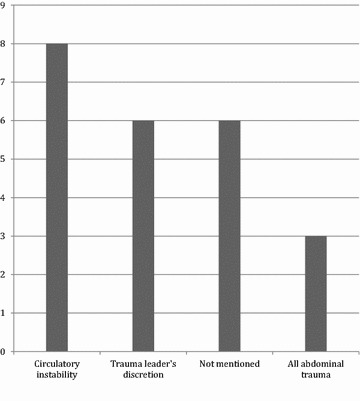
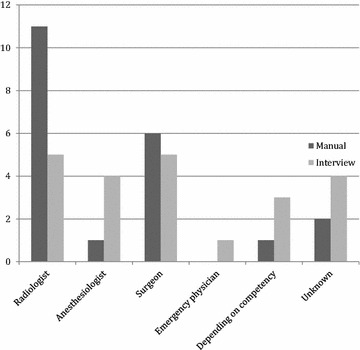
Results: Guidelines were obtained from all 22 hospitals receiving traumatized patients in Denmark. Twenty-one (95.5%) of the guidelines included and recommended FAST as part of trauma assessment. The recommended person to perform the examination was the radiologist in n = 11 (50.0%), the surgeon in n = 6 (27.3%), the anesthesiologist in n = 1 (4.5%), and unspecified in n = 3 (13.6%) facilities. FAST indications varied between circulatory instability n = 8 (36.4%), team leader's discretion n = 6 (27.3%), abdominal trauma n = 3 (13.6%), and not specified n = 6 (27.3%). Telephone interviews revealed that exams were always n = 8 (36.4%) or often n = 4 (18.2%) registered in the patients' charts. The remaining n = 10 (45.5%) facilities either never registered n = 2 (9.1%), it was not possible to register n = 1 (4.5%), or unknown by the trauma leaders n = 7 (31.8%). Images were often stored in n = 1 (4.5%), never stored in n = 10 (45.5%), not possible to store in n = 2 (9.1%), and unknown in n = 9 (40.9%) facilities.
Conclusion: Ultrasonography was used in a non-uniform fashion by multiple specialties in Danish trauma facilities. Very few images from FAST examinations were stored and documentation was scanty. National guidelines on application and documentation of ultrasonography in trauma are called for.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
