{"title":"从血液和呼吸道同时分离黄杆菌:印度首例报告。","authors":"Vidhi Jain, Nayani Amrin Fatema Afzal Hussain, Tasneem Siddiqui, Chinmoy Sahu, Malay Ghar, Kashi Nath Prasad","doi":"10.1099/jmmcr.0.005122","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction.</b> Species of the genus <i>Chryseobacterium</i> are emerging healthcare-associated pathogens, often colonizing the hospital environment. There are no clear guidelines available for antimicrobial susceptibility of this organism. In this report we present the first case, to our knowledge, of simultaneous central-line-associated bloodstream infection (CLABSI) and ventilator-associated pneumonia (VAP) due to <i>Chryseobacterium gleum</i> from India. <b>Case presentation.</b> A 62 years old man with a history of a road traffic accident 1 month previously was referred to our center for further management. He developed features of sepsis and aspiration pneumonia on day 3 of admission. Four blood cultures (two each from central and peripheral lines) and two tracheal aspirate cultures grew pure yellow colonies of bacteria. Both matrix assisted laser desorption ionization time of flight mass spectrometry, (MALDI-TOF MS; bioMérieux, Marcy-L'Etoile, France,) and BD Phoenix (BD Biosciences, Maryland, USA) identified the organism as <i>C. gleum</i>. However, BD Phoenix failed to provide MIC breakpoints. The isolates of <i>C. gleum</i> both from blood and tracheal aspirate showed identical susceptibility patterns: resistant to cephalosporins and carbapenems and susceptible to ciprofloxacin, levofloxacin, amikacin, trimethoprim+sulfamethoxazole, piperacillin-tazobactam, cefoperazone-sulbactam, doxycycline, minocycline and vancomycin. Following levofloxacin therapy, the fever responded within 48 h and procalcitonin levels decreased without removal of the central line or endotracheal tube. However, the patient developed sudden cardiac arrest on day 10 of treatment and could not be resuscitated. <b>Conclusion.</b> Rapid and accurate identification of <i>C. gleum</i> in the laboratory, preferably based on MALDI-TOF, is essential for guiding therapy. <i>C. gleum</i> responds well to fluoroquinolones without the need to remove indwelling catheters.</p>","PeriodicalId":73559,"journal":{"name":"JMM case reports","volume":"4 10","pages":"e005122"},"PeriodicalIF":0.0000,"publicationDate":"2017-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5692238/pdf/","citationCount":"14","resultStr":"{\"title\":\"Simultaneous isolation of <i>Chryseobacterium gleum</i> from bloodstream and respiratory tract: first case report from India.\",\"authors\":\"Vidhi Jain, Nayani Amrin Fatema Afzal Hussain, Tasneem Siddiqui, Chinmoy Sahu, Malay Ghar, Kashi Nath Prasad\",\"doi\":\"10.1099/jmmcr.0.005122\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction.</b> Species of the genus <i>Chryseobacterium</i> are emerging healthcare-associated pathogens, often colonizing the hospital environment. There are no clear guidelines available for antimicrobial susceptibility of this organism. In this report we present the first case, to our knowledge, of simultaneous central-line-associated bloodstream infection (CLABSI) and ventilator-associated pneumonia (VAP) due to <i>Chryseobacterium gleum</i> from India. <b>Case presentation.</b> A 62 years old man with a history of a road traffic accident 1 month previously was referred to our center for further management. He developed features of sepsis and aspiration pneumonia on day 3 of admission. Four blood cultures (two each from central and peripheral lines) and two tracheal aspirate cultures grew pure yellow colonies of bacteria. Both matrix assisted laser desorption ionization time of flight mass spectrometry, (MALDI-TOF MS; bioMérieux, Marcy-L'Etoile, France,) and BD Phoenix (BD Biosciences, Maryland, USA) identified the organism as <i>C. gleum</i>. However, BD Phoenix failed to provide MIC breakpoints. The isolates of <i>C. gleum</i> both from blood and tracheal aspirate showed identical susceptibility patterns: resistant to cephalosporins and carbapenems and susceptible to ciprofloxacin, levofloxacin, amikacin, trimethoprim+sulfamethoxazole, piperacillin-tazobactam, cefoperazone-sulbactam, doxycycline, minocycline and vancomycin. Following levofloxacin therapy, the fever responded within 48 h and procalcitonin levels decreased without removal of the central line or endotracheal tube. However, the patient developed sudden cardiac arrest on day 10 of treatment and could not be resuscitated. <b>Conclusion.</b> Rapid and accurate identification of <i>C. gleum</i> in the laboratory, preferably based on MALDI-TOF, is essential for guiding therapy. <i>C. gleum</i> responds well to fluoroquinolones without the need to remove indwelling catheters.</p>\",\"PeriodicalId\":73559,\"journal\":{\"name\":\"JMM case reports\",\"volume\":\"4 10\",\"pages\":\"e005122\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-10-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5692238/pdf/\",\"citationCount\":\"14\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMM case reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1099/jmmcr.0.005122\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1099/jmmcr.0.005122","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Simultaneous isolation of Chryseobacterium gleum from bloodstream and respiratory tract: first case report from India.
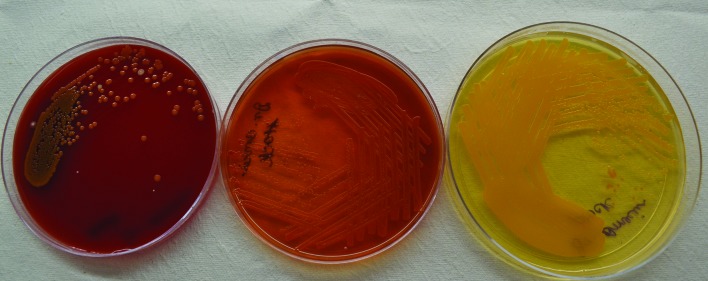
Introduction. Species of the genus Chryseobacterium are emerging healthcare-associated pathogens, often colonizing the hospital environment. There are no clear guidelines available for antimicrobial susceptibility of this organism. In this report we present the first case, to our knowledge, of simultaneous central-line-associated bloodstream infection (CLABSI) and ventilator-associated pneumonia (VAP) due to Chryseobacterium gleum from India. Case presentation. A 62 years old man with a history of a road traffic accident 1 month previously was referred to our center for further management. He developed features of sepsis and aspiration pneumonia on day 3 of admission. Four blood cultures (two each from central and peripheral lines) and two tracheal aspirate cultures grew pure yellow colonies of bacteria. Both matrix assisted laser desorption ionization time of flight mass spectrometry, (MALDI-TOF MS; bioMérieux, Marcy-L'Etoile, France,) and BD Phoenix (BD Biosciences, Maryland, USA) identified the organism as C. gleum. However, BD Phoenix failed to provide MIC breakpoints. The isolates of C. gleum both from blood and tracheal aspirate showed identical susceptibility patterns: resistant to cephalosporins and carbapenems and susceptible to ciprofloxacin, levofloxacin, amikacin, trimethoprim+sulfamethoxazole, piperacillin-tazobactam, cefoperazone-sulbactam, doxycycline, minocycline and vancomycin. Following levofloxacin therapy, the fever responded within 48 h and procalcitonin levels decreased without removal of the central line or endotracheal tube. However, the patient developed sudden cardiac arrest on day 10 of treatment and could not be resuscitated. Conclusion. Rapid and accurate identification of C. gleum in the laboratory, preferably based on MALDI-TOF, is essential for guiding therapy. C. gleum responds well to fluoroquinolones without the need to remove indwelling catheters.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
